{"title":"Leg mouse: “Tennis leg”","authors":"Siddhi Chawla","doi":"10.1002/ird3.59","DOIUrl":null,"url":null,"abstract":"<p>A 25-year-old male presented to the orthopedic out-patient department with a small bulge on the back of the left lower leg which appears on the plantarflexion of the foot. It developed suddenly 5 days ago when the patient was running with a sharp pain in the calf (Figure 1a). On examination, there was a well-defined soft tissue density lesion in the medial side of the leg which became more pronounced on plantarflexion (Video S1). Ultrasound (done on Sonoscape P12) with a linear probe (9–12 Hz) revealed a bulky medial head of gastrocnemius with lobulated inferior edge contour at the site of the swelling with hyperechoic soft tissue at the inferior edge of the belly signifying buckled up aponeurosis at its inferior edge (Figure 1b,c; Video S2 shows the dynamic evaluation of gastrocnemius with curvilinear probe; Video S3 shows the normal contralateral side for comparison). The muscle became prominent on plantar flexion with increase in the buckling of the aponeurosis. The swelling disappeared on the dorsiflexion and on ultrasound findings returned to baseline. There was no intermuscular fluid or adjacent collection. A diagnosis of “Tennis leg” due to a partial rupture of the medial head of gastrocnemius at musculoaponeurosis junction was made.</p><p>“Tennis leg” is commonly seen in middle-aged persons and is a common sports-related injury or chronic stress due to strenuous exercise commonly occurs following the extension of the knee and forced dorsiflexion of the ankle because of playing tennis or activities such as jumping or running with “push-off” [<span>1</span>]. Other causes of “Tennis leg” include plantaris tendon rupture, partial rupture of soleus, fluid between the gastrocnemius and soleus muscles without the evidence of muscle injury, and even deep vein thrombosis [<span>2</span>]. Ultrasound is the first imaging modality of choice to look at the nature of lesion, exact location, place of origin, and differentiate muscular pathologies based on their location from other masses. It can also detect the deep vein thrombosis which appears as echogenic, non-compressible, thrombus within deep or superficial veins. Dynamic ultrasound adds to static imaging in cases with muscular injury by giving us a real time opportunity to assess the muscle and its relative movement with common maneuvers; like plantar and dorsiflexion in our case. Magnetic resonance imaging (MRI) is needed in cases where ultrasound is not able to localize or characterize the pathology. It helps us to differentiate gastrocnemius tear from other musculotendinous tears which can present similarly based on their location and much early than the ultrasound. It is also used in cases that require operative management to look at its operability with respect to grading of injury, any additional injuries and preoperative planning for reconstruction of tendons if required. In our case however, MRI was not performed in view of the partial tear of gastrocnemius documented on ultrasound. In such cases, prospects for recovery are good. Nonoperative management with staged physiotherapy involving gradual weight-bearing over weeks is the standard of care in such cases. Similar injuries in athletes might require surgical repair [<span>3</span>]. Our patient was treated with nonsteroidal anti-inflammatory drugs and physiotherapy. At 2 months follow-up, pain and deformity had decreased and he was able to carry out his routine activities; however, he was still not able to run.</p><p><b>Siddhi Chawla</b>: Initial draft; concept; revision; editing; review.</p><p>The author declares no conflict of interest.</p><p>This article is a practice-oriented case study description that made extensive use of secondary information sources and also drew upon the professional knowledge of the author. Therefore, the creation of this case study article did not involve any formal research study. In addition, all images and videos included were after patients informed consent. Hence, IRB review was not required for this article.</p><p>All patients provided written informed consent at the time of entering this study.</p>","PeriodicalId":73508,"journal":{"name":"iRadiology","volume":"2 2","pages":"222-224"},"PeriodicalIF":0.0000,"publicationDate":"2024-02-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.59","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"iRadiology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ird3.59","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
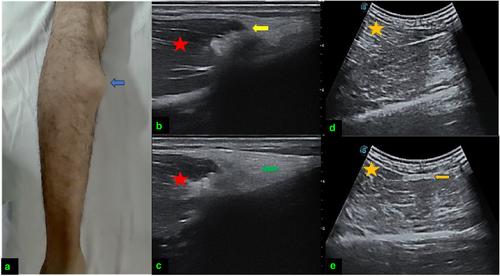
A 25-year-old male presented to the orthopedic out-patient department with a small bulge on the back of the left lower leg which appears on the plantarflexion of the foot. It developed suddenly 5 days ago when the patient was running with a sharp pain in the calf (Figure 1a). On examination, there was a well-defined soft tissue density lesion in the medial side of the leg which became more pronounced on plantarflexion (Video S1). Ultrasound (done on Sonoscape P12) with a linear probe (9–12 Hz) revealed a bulky medial head of gastrocnemius with lobulated inferior edge contour at the site of the swelling with hyperechoic soft tissue at the inferior edge of the belly signifying buckled up aponeurosis at its inferior edge (Figure 1b,c; Video S2 shows the dynamic evaluation of gastrocnemius with curvilinear probe; Video S3 shows the normal contralateral side for comparison). The muscle became prominent on plantar flexion with increase in the buckling of the aponeurosis. The swelling disappeared on the dorsiflexion and on ultrasound findings returned to baseline. There was no intermuscular fluid or adjacent collection. A diagnosis of “Tennis leg” due to a partial rupture of the medial head of gastrocnemius at musculoaponeurosis junction was made.
“Tennis leg” is commonly seen in middle-aged persons and is a common sports-related injury or chronic stress due to strenuous exercise commonly occurs following the extension of the knee and forced dorsiflexion of the ankle because of playing tennis or activities such as jumping or running with “push-off” [1]. Other causes of “Tennis leg” include plantaris tendon rupture, partial rupture of soleus, fluid between the gastrocnemius and soleus muscles without the evidence of muscle injury, and even deep vein thrombosis [2]. Ultrasound is the first imaging modality of choice to look at the nature of lesion, exact location, place of origin, and differentiate muscular pathologies based on their location from other masses. It can also detect the deep vein thrombosis which appears as echogenic, non-compressible, thrombus within deep or superficial veins. Dynamic ultrasound adds to static imaging in cases with muscular injury by giving us a real time opportunity to assess the muscle and its relative movement with common maneuvers; like plantar and dorsiflexion in our case. Magnetic resonance imaging (MRI) is needed in cases where ultrasound is not able to localize or characterize the pathology. It helps us to differentiate gastrocnemius tear from other musculotendinous tears which can present similarly based on their location and much early than the ultrasound. It is also used in cases that require operative management to look at its operability with respect to grading of injury, any additional injuries and preoperative planning for reconstruction of tendons if required. In our case however, MRI was not performed in view of the partial tear of gastrocnemius documented on ultrasound. In such cases, prospects for recovery are good. Nonoperative management with staged physiotherapy involving gradual weight-bearing over weeks is the standard of care in such cases. Similar injuries in athletes might require surgical repair [3]. Our patient was treated with nonsteroidal anti-inflammatory drugs and physiotherapy. At 2 months follow-up, pain and deformity had decreased and he was able to carry out his routine activities; however, he was still not able to run.
This article is a practice-oriented case study description that made extensive use of secondary information sources and also drew upon the professional knowledge of the author. Therefore, the creation of this case study article did not involve any formal research study. In addition, all images and videos included were after patients informed consent. Hence, IRB review was not required for this article.
All patients provided written informed consent at the time of entering this study.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
