Post-stem cell transplant maintenance in FLT3mut acute myeloid leukemia – A retrospective analysis: Outcomes are improved with midostaurin but not with gilteritinib
Karam Ashouri, Krithika Chennapan, Anastasia Martynova, Samvel Nazaretyan, Amir Ali, Anush Aram Ginosyan, Eric Tam, Abdullah Ladha, Karrune Woan, Preet Chaudhary, Imran Siddiqi, George Yaghmour
{"title":"Post-stem cell transplant maintenance in FLT3mut acute myeloid leukemia – A retrospective analysis: Outcomes are improved with midostaurin but not with gilteritinib","authors":"Karam Ashouri, Krithika Chennapan, Anastasia Martynova, Samvel Nazaretyan, Amir Ali, Anush Aram Ginosyan, Eric Tam, Abdullah Ladha, Karrune Woan, Preet Chaudhary, Imran Siddiqi, George Yaghmour","doi":"10.1002/jha2.885","DOIUrl":null,"url":null,"abstract":"<p>The FMS-like tyrosine kinase 3 (<i>FLT3</i>) domain is the most mutated gene in acute myeloid leukemia (AML), with FLT3 internal tandem duplication (ITD) mutations conferring adverse outcomes [<span>1, 2</span>]. Maintenance therapy after hematopoietic stem cell transplant (HSCT) may be essential, as FLT3 AML patients experience high rates of post-HSCT relapse and mortality [<span>3</span>]. Terao et al. found that relapsed/refractory (R/R) FLT3 AML patients who received post-HSCT maintenance gilteritinib had improved overall survival (OS) (1-year OS, 100% vs. 45.5%, <i>p</i> = 0.0075) and cumulative incidence of relapse (CIR, 1-year CIR 0% vs. 68.8%, <i>p</i> = 0.0028) [<span>4</span>]. However, the phase 3 MORPHO trial failed to reach the primary outcome of improved relapse-free survival (RFS) with post-HSCT maintenance gilteritinib compared to placebo in FLT3-ITD AML patients except in measurable residual disease (MRD) positive patients [<span>5</span>]. As prospective data on FLT3 inhibitor maintenance therapy are evolving, there is a need to investigate real-life data and outcomes to guide clinical decisions. </p><p>We retrospectively studied adult patients with FLT3 AML treated at the University of Southern California (USC) Norris Cancer Center between May 2017 and July 2022. This study was approved by USC's Institutional Review Board, and data were retrieved from the Norris Comprehensive Cancer Center's electronic medical record system. </p><p>We found post-HSCT maintenance therapy with FLT3 inhibitors improved OS, with a 2-year OS of 96.2% (93.3% for gilteritinib and 100% for midostaurin). The RADIUS trial reported a lower 2-year OS of 85% with midostaurin maintenance, while SORMAIN reported 90.5% OS with sorafenib maintenance [<span>6, 7</span>]. Our 2-year RFS with FLT3 maintenance was 89.7% (88.9% for gilteritinib and 90.9% for midostaurin), whereas both RADIUS and SORMAIN trials reported 2-year RFS of 85%. The RADIUS study exclusively included patients with FLT3-ITD mutations, which have poorer prognosis and may have contributed to worse outcomes than our study population (75% ITD and 25% TKD). However, our cohort included R/R AML patients and post-HSCT maintenance with both midostaurin and gilteritinib, while the RADIUS population was exclusively in CR1 and used only post-HSCT midostaurin. This is significant because neither our R/R patients nor our post-HSCT gilteritinib patients had statistically significant improved survival. Therefore, survival benefit was exclusively derived from patients in CR1 and who received midostaurin.</p><p>Terao et al. found a survival benefit of gilteritinib maintenance in the post-HSCT setting. The ADMIRAL trial also found a survival benefit for gilteritinib in R/R FLT3 AML, though less pronounced than Terao's, with only 40% achieving RFS [<span>8, 9</span>]. Contrastingly, our study found a survival benefit with post-HSCT midostaurin maintenance but no benefit with gilteritinib. Possibly explaining this difference, post-HSCT maintenance therapy initiation occurred later in our study, with a median of D+104 compared to D+55 in the ADMIRAL trial and D+36 in Terao's study. Terao proposes that early initiation of gilteritinib may augment the graft-versus-leukemia effect, which may yield improved survival outcomes in their study compared to others using post-HSCT maintenance. However, this phenomenon has only been suggested in pre-clinical studies so far [<span>10</span>]. Given the uncertainty regarding the optimal timing of FLT3 inhibitor maintenance therapy, delayed initiation of gilteritinib in our cohort possibly eliminated survival benefits. Our retrospective study demonstrates improved OS and RFS with post-HSCT midostaurin maintenance therapy in FLT3-positive AML. Further studies are required to elucidate which patients are likely to benefit from maintenance therapy with FLT3 inhibitors.</p><p>This observational study with a limited sample of patients reflects single-center practice. The treating clinician decided administration of maintenance FLT3 inhibitor therapy, the choice of inhibitor, and the dose and timing of initiation. Additionally, donor factors may have affected outcomes in the study population but were not evaluated in this study.</p><p>All authors participated in study design, data acquisition, analysis, or interpretation of data, and contributed to manuscript writing and reviewing. All authors approved the final version of the manuscript.</p><p>George Yaghmour Speakers Bureau: Jazz, Incyte, Astellas, BMS, Secura bio, blueprint, SOBI, Karius, Kite, Celgene, AbbVie, Rigel, Servier, GSK, Takeda, and Pfizer Advisory Board: Gilead, Alexion, Pfizer, AbbVie, and Servier</p><p>Not applicable</p><p>Not applicable</p><p>This study was IRB-exempt from patient consent due to its retrospective nature.</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>","PeriodicalId":72883,"journal":{"name":"EJHaem","volume":"5 2","pages":"423-427"},"PeriodicalIF":1.2000,"publicationDate":"2024-04-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.885","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EJHaem","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jha2.885","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
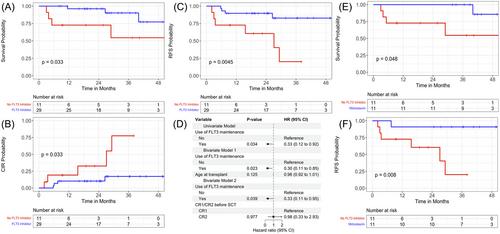
The FMS-like tyrosine kinase 3 (FLT3) domain is the most mutated gene in acute myeloid leukemia (AML), with FLT3 internal tandem duplication (ITD) mutations conferring adverse outcomes [1, 2]. Maintenance therapy after hematopoietic stem cell transplant (HSCT) may be essential, as FLT3 AML patients experience high rates of post-HSCT relapse and mortality [3]. Terao et al. found that relapsed/refractory (R/R) FLT3 AML patients who received post-HSCT maintenance gilteritinib had improved overall survival (OS) (1-year OS, 100% vs. 45.5%, p = 0.0075) and cumulative incidence of relapse (CIR, 1-year CIR 0% vs. 68.8%, p = 0.0028) [4]. However, the phase 3 MORPHO trial failed to reach the primary outcome of improved relapse-free survival (RFS) with post-HSCT maintenance gilteritinib compared to placebo in FLT3-ITD AML patients except in measurable residual disease (MRD) positive patients [5]. As prospective data on FLT3 inhibitor maintenance therapy are evolving, there is a need to investigate real-life data and outcomes to guide clinical decisions.
We retrospectively studied adult patients with FLT3 AML treated at the University of Southern California (USC) Norris Cancer Center between May 2017 and July 2022. This study was approved by USC's Institutional Review Board, and data were retrieved from the Norris Comprehensive Cancer Center's electronic medical record system.
We found post-HSCT maintenance therapy with FLT3 inhibitors improved OS, with a 2-year OS of 96.2% (93.3% for gilteritinib and 100% for midostaurin). The RADIUS trial reported a lower 2-year OS of 85% with midostaurin maintenance, while SORMAIN reported 90.5% OS with sorafenib maintenance [6, 7]. Our 2-year RFS with FLT3 maintenance was 89.7% (88.9% for gilteritinib and 90.9% for midostaurin), whereas both RADIUS and SORMAIN trials reported 2-year RFS of 85%. The RADIUS study exclusively included patients with FLT3-ITD mutations, which have poorer prognosis and may have contributed to worse outcomes than our study population (75% ITD and 25% TKD). However, our cohort included R/R AML patients and post-HSCT maintenance with both midostaurin and gilteritinib, while the RADIUS population was exclusively in CR1 and used only post-HSCT midostaurin. This is significant because neither our R/R patients nor our post-HSCT gilteritinib patients had statistically significant improved survival. Therefore, survival benefit was exclusively derived from patients in CR1 and who received midostaurin.
Terao et al. found a survival benefit of gilteritinib maintenance in the post-HSCT setting. The ADMIRAL trial also found a survival benefit for gilteritinib in R/R FLT3 AML, though less pronounced than Terao's, with only 40% achieving RFS [8, 9]. Contrastingly, our study found a survival benefit with post-HSCT midostaurin maintenance but no benefit with gilteritinib. Possibly explaining this difference, post-HSCT maintenance therapy initiation occurred later in our study, with a median of D+104 compared to D+55 in the ADMIRAL trial and D+36 in Terao's study. Terao proposes that early initiation of gilteritinib may augment the graft-versus-leukemia effect, which may yield improved survival outcomes in their study compared to others using post-HSCT maintenance. However, this phenomenon has only been suggested in pre-clinical studies so far [10]. Given the uncertainty regarding the optimal timing of FLT3 inhibitor maintenance therapy, delayed initiation of gilteritinib in our cohort possibly eliminated survival benefits. Our retrospective study demonstrates improved OS and RFS with post-HSCT midostaurin maintenance therapy in FLT3-positive AML. Further studies are required to elucidate which patients are likely to benefit from maintenance therapy with FLT3 inhibitors.
This observational study with a limited sample of patients reflects single-center practice. The treating clinician decided administration of maintenance FLT3 inhibitor therapy, the choice of inhibitor, and the dose and timing of initiation. Additionally, donor factors may have affected outcomes in the study population but were not evaluated in this study.
All authors participated in study design, data acquisition, analysis, or interpretation of data, and contributed to manuscript writing and reviewing. All authors approved the final version of the manuscript.
George Yaghmour Speakers Bureau: Jazz, Incyte, Astellas, BMS, Secura bio, blueprint, SOBI, Karius, Kite, Celgene, AbbVie, Rigel, Servier, GSK, Takeda, and Pfizer Advisory Board: Gilead, Alexion, Pfizer, AbbVie, and Servier
Not applicable
Not applicable
This study was IRB-exempt from patient consent due to its retrospective nature.
The authors have confirmed clinical trial registration is not needed for this submission.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
