Marc Hohenhaus, Jan-Helge Klingler, Christoph Scholz, Ralf Watzlawick, Ulrich Hubbe, Jürgen Beck, Marco Reisert, Urs Würtemberger, Nico Kremers, Katharina Wolf
{"title":"Quantification of cervical spinal stenosis by automated 3D MRI segmentation of spinal cord and cerebrospinal fluid space","authors":"Marc Hohenhaus, Jan-Helge Klingler, Christoph Scholz, Ralf Watzlawick, Ulrich Hubbe, Jürgen Beck, Marco Reisert, Urs Würtemberger, Nico Kremers, Katharina Wolf","doi":"10.1038/s41393-024-00993-8","DOIUrl":null,"url":null,"abstract":"Prospective diagnostic study. Anatomical evaluation and graduation of the severity of spinal stenosis is essential in degenerative cervical spine disease. In clinical practice, this is subjectively categorized on cervical MRI lacking an objective and reliable classification. We implemented a fully-automated quantification of spinal canal compromise through 3D T2-weighted MRI segmentation. Medical Center - University of Freiburg, Germany. Evaluation of 202 participants receiving 3D T2-weighted MRI of the cervical spine. Segments C2/3 to C6/7 were analyzed for spinal cord and cerebrospinal fluid space volume through a fully-automated segmentation based on a trained deep convolutional neural network. Spinal canal narrowing was characterized by relative values, across sever segments as adapted Maximal Canal Compromise (aMCC), and within the index segment as adapted Spinal Cord Occupation Ratio (aSCOR). Additionally, all segments were subjectively categorized by three observers as “no”, “relative” or “absolute” stenosis. Computed scores were applied on the subjective categorization. 798 (79.0%) segments were subjectively categorized as “no” stenosis, 85 (8.4%) as “relative” stenosis, and 127 (12.6%) as “absolute” stenosis. The calculated scores revealed significant differences between each category (p ≤ 0.001). Youden’s Index analysis of ROC curves revealed optimal cut-offs to distinguish between “no” and “relative” stenosis for aMCC = 1.18 and aSCOR = 36.9%, and between “relative” and “absolute” stenosis for aMCC = 1.54 and aSCOR = 49.3%. The presented fully-automated segmentation algorithm provides high diagnostic accuracy and objective classification of cervical spinal stenosis. The calculated cut-offs can be used for convenient radiological quantification of the severity of spinal canal compromise in clinical routine.","PeriodicalId":21976,"journal":{"name":"Spinal cord","volume":"62 7","pages":"371-377"},"PeriodicalIF":2.2000,"publicationDate":"2024-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.nature.com/articles/s41393-024-00993-8.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spinal cord","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41393-024-00993-8","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
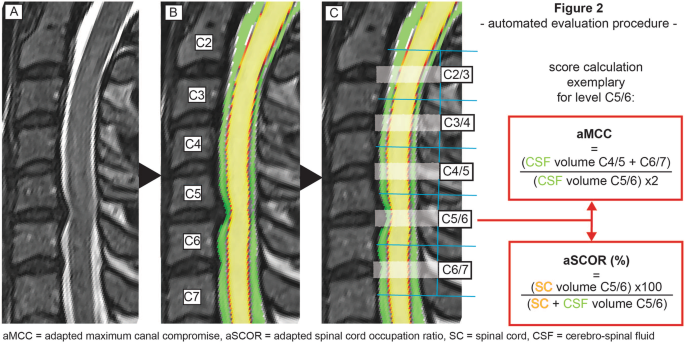
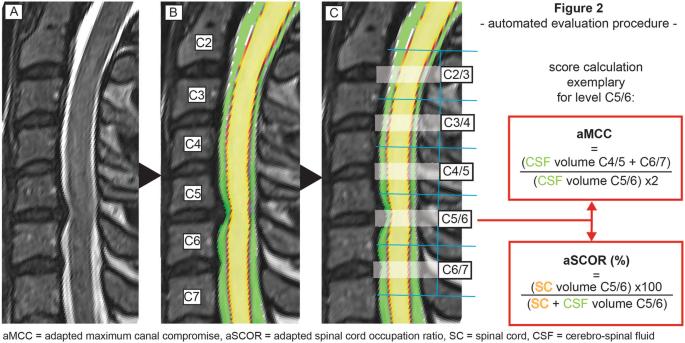
Prospective diagnostic study. Anatomical evaluation and graduation of the severity of spinal stenosis is essential in degenerative cervical spine disease. In clinical practice, this is subjectively categorized on cervical MRI lacking an objective and reliable classification. We implemented a fully-automated quantification of spinal canal compromise through 3D T2-weighted MRI segmentation. Medical Center - University of Freiburg, Germany. Evaluation of 202 participants receiving 3D T2-weighted MRI of the cervical spine. Segments C2/3 to C6/7 were analyzed for spinal cord and cerebrospinal fluid space volume through a fully-automated segmentation based on a trained deep convolutional neural network. Spinal canal narrowing was characterized by relative values, across sever segments as adapted Maximal Canal Compromise (aMCC), and within the index segment as adapted Spinal Cord Occupation Ratio (aSCOR). Additionally, all segments were subjectively categorized by three observers as “no”, “relative” or “absolute” stenosis. Computed scores were applied on the subjective categorization. 798 (79.0%) segments were subjectively categorized as “no” stenosis, 85 (8.4%) as “relative” stenosis, and 127 (12.6%) as “absolute” stenosis. The calculated scores revealed significant differences between each category (p ≤ 0.001). Youden’s Index analysis of ROC curves revealed optimal cut-offs to distinguish between “no” and “relative” stenosis for aMCC = 1.18 and aSCOR = 36.9%, and between “relative” and “absolute” stenosis for aMCC = 1.54 and aSCOR = 49.3%. The presented fully-automated segmentation algorithm provides high diagnostic accuracy and objective classification of cervical spinal stenosis. The calculated cut-offs can be used for convenient radiological quantification of the severity of spinal canal compromise in clinical routine.
期刊介绍:
Spinal Cord is a specialised, international journal that has been publishing spinal cord related manuscripts since 1963. It appears monthly, online and in print, and accepts contributions on spinal cord anatomy, physiology, management of injury and disease, and the quality of life and life circumstances of people with a spinal cord injury. Spinal Cord is multi-disciplinary and publishes contributions across the entire spectrum of research ranging from basic science to applied clinical research. It focuses on high quality original research, systematic reviews and narrative reviews.
Spinal Cord''s sister journal Spinal Cord Series and Cases: Clinical Management in Spinal Cord Disorders publishes high quality case reports, small case series, pilot and retrospective studies perspectives, Pulse survey articles, Point-couterpoint articles, correspondences and book reviews. It specialises in material that addresses all aspects of life for persons with spinal cord injuries or disorders. For more information, please see the aims and scope of Spinal Cord Series and Cases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
