The fundamental role of the renin–angiotensin–aldosterone system in the pathophysiology of chronic kidney disease, congestive heart failure, hypertension and proteinuria is well established in pre-clinical and clinical studies. Mineralocorticoid receptor antagonists are among the primary options for renin–angiotensin–aldosterone system blockage, along with angiotensin-converting enzyme inhibitors and angiotensin receptor blockers.
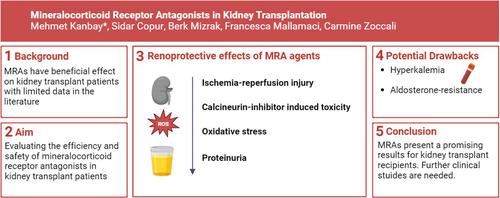
In this narrative review, we aim to evaluate the efficiency and safety of mineralocorticoid receptor antagonists in kidney transplant recipients, including the potential underlying pathophysiology.
The efficiency and safety of mineralocorticoid receptor antagonists in managing chronic kidney disease and proteinuria, either non-nephrotic or nephrotic range, have been demonstrated among nontransplanted patients, though studies investigating the role of mineralocorticoid receptor antagonists among kidney transplant recipients are scarce. Nevertheless, promising results have been reported in pre-clinical and clinical studies among kidney transplant recipients regarding the role of mineralocorticoid receptor antagonists in terms of ischaemia–reperfusion injury, proteinuria, or calcineurin inhibitor-mediated nephrotoxicity without considerable adverse events such as hypotension, hyperkalaemia or worsening renal functions.
Even though initial results regarding the role of mineralocorticoid receptor antagonist therapy for kidney transplant recipients are promising, there is clear need for large-scale randomized clinical trials with long-term follow-up data.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
