2024 guidelines for the vaccination of dogs and cats – compiled by the Vaccination Guidelines Group (VGG) of the World Small Animal Veterinary Association (WSAVA)
R. A. Squires, C. Crawford, M. Marcondes, N. Whitley
{"title":"2024 guidelines for the vaccination of dogs and cats – compiled by the Vaccination Guidelines Group (VGG) of the World Small Animal Veterinary Association (WSAVA)","authors":"R. A. Squires, C. Crawford, M. Marcondes, N. Whitley","doi":"10.1111/jsap.13718","DOIUrl":null,"url":null,"abstract":"<p>The World Small Animal Veterinary Association (WSAVA) Vaccination Guidelines Group (VGG) was convened to develop guidelines for the vaccination of dogs and cats intended to be helpful to veterinarians globally. Previous guidelines, published in 2007, 2010 and 2016, have been cited in the peer-reviewed scientific literature several hundred times and downloaded tens of thousands of times. The present document is an updated version of these guidelines. The VGG recognises that its recommendations must be broad and based on fundamental immunological principles because detailed recommendations about vaccines and vaccination of dogs and cats that might be suitable for some countries or regions may be much less applicable elsewhere.</p><p>Guidelines are intended to provide broad guidance for veterinarians in decision-making. They do not describe mandatory or minimum standards of care. These guidelines can be used by national and regional veterinary associations and individual veterinarians or veterinary practices to develop their own vaccination schedules suitable to their own local conditions. Notwithstanding this, the VGG strongly recommends that ALL dogs and cats should receive the benefit of vaccination. This will not only protect individual animals but will improve “herd immunity” to help minimise the risk of contagious disease outbreaks.</p><p>With this background in mind, the VGG has defined <i>core vaccines</i> as those that ALL dogs and cats should receive, after considering their lifestyle and the geographical areas in which they live or to which they travel. Some core vaccines protect animals from potentially life-threatening diseases that have global distribution while others protect against life-threatening diseases that are prevalent only in particular countries or regions. Core vaccines for dogs <i>in all parts of the world</i> are those that protect against canine distemper virus (CDV), canine adenovirus type 1 (CAV) and canine parvovirus type 2 (CPV). Core vaccines for cats in all parts of the world are those that protect against feline parvovirus (FPV), feline calicivirus (FCV) and feline herpesvirus-1 (FHV). In areas of the world where rabies is endemic, vaccination against rabies virus should be considered essential for both dogs and cats (<i>i.e</i>. rabies vaccines are <i>core</i> in those places), even if there is no legal requirement for this. Leptospirosis in dogs is another life-threatening, zoonotic disease that is widely distributed around the world. In countries or regions where canine leptospirosis is endemic, where implicated serogroups are known and where suitable vaccines are available, vaccination of all dogs against leptospirosis is highly recommended and the vaccines should be considered <i>core</i> in those places. In many parts of the world, feline leukaemia virus (FeLV)-related diseases are endemic. In these places, FeLV vaccines should be considered <i>core</i> for young cats (<1 year of age) and for adult cats with outdoor access or that live with other cats that have outdoor access.</p><p>The VGG recognises that maternally derived antibodies (MDAs) interfere substantially with the efficacy of most currently available core vaccines that are administered to puppies and kittens early in life (protecting against CDV, CAV and CPV in puppies, FPV, FCV and FHV in kittens). As the level of MDA varies substantially within and between litters, VGG recommends the administration of multiple core vaccine doses to puppies and kittens, every 2 to 4 weeks, with the final dose being delivered at 16 weeks of age or older. In situations where a puppy or kitten can only receive a single vaccination (<i>e.g</i>. in the case of cost constraints), vaccination should be with the core vaccines at 16+ weeks of age. Revaccination at or after 26 weeks of age (rather than waiting until 12 to 16 months of age) is advised to immunise without unnecessary delay the minority of animals that may still have had interfering MDA present at the time of their 16+ week vaccination.</p><p>The VGG supports the use of serological testing from 20 weeks of age onwards to detect seroconversion (to CDV, CAV and CPV in dogs and FPV in cats) following vaccination. This can help confirm active immune protection in young and young adult animals, help optimise revaccination intervals in mature adult animals, and in some situations, can help in the management of contagious disease outbreaks in shelters.</p><p>Vaccines should not be given needlessly. Core vaccines should not be given any more frequently than necessary in adult animals. There is an abundance of peer-reviewed, published evidence showing that the duration of immunity (DOI) provided by most, modern, modified live virus (MLV) core vaccines is many years.</p><p>The VGG has defined <i>non-core vaccines</i> as those that should be highly recommended in animals whose geographical location and/or lifestyle (<i>e.g</i>. indoor-outdoor access, multi-pet household) places them at risk of contracting particular infections not designated as core. A careful conversation between veterinarian and owner is needed to inform the decision about which non-core vaccines to recommend for each patient. The VGG has classified some vaccines as <i>not recommended</i> where there is insufficient scientific evidence to justify recommending their use anywhere. The VGG has not considered a few “minor” vaccine products that have very restricted geographical availability or applicability.</p><p>The VGG strongly encourages veterinarians to educate their clients about the value of regular health checks (usually annual, sometimes more often) as opposed to speaking of “vaccination consultations.” The annual health check is much more than just a vaccination consultation, although it will often include administration of selected vaccines that need to be administered annually. The DOI provided by most non-core vaccines is about 1 year.</p><p>Veterinarians are also encouraged to undergo training intended to improve the experience of pets, owners and veterinary staff before and during pet health check visits. The Free Fear training programme (https://fearfreepets.com/fear-free-certification-overview/) and the Cat Friendly Certificate programme (https://catvets.com/cfp/cat-friendly-certificate-program/) are examples.</p><p>The VGG has considered the use of vaccines in shelters and sanctuaries, again recognising the financial constraints under which some of these facilities operate. The VGG minimum shelter guidelines state that all dogs and cats entering such establishments should be vaccinated before, or at the time of their entry, with the core MLV vaccines. Where finances permit, these vaccines should be administered every 2 to 3 weeks starting at 4 weeks of age and continuing until 5 months of age. Vaccines against respiratory disease are considered non-core for pet dogs living in typical homes but should be considered core for shelter-housed dogs.</p><p>The VGG recognises the importance of adverse reaction reporting schemes but understands that these are variably developed in different countries. Veterinarians are strongly encouraged to report all possible adverse events to the manufacturer and to the regulatory authority to expand the knowledge base that drives development of improved, safer vaccines.</p><p>The WSAVA VGG was convened in 2006 to develop guidelines for the vaccination of dogs and cats intended to be helpful to veterinarians globally. Previous guidelines were published in 2007 (Day, Horzinek & Schultz <span>2007a</span>), 2010 (Day et al., <span>2010</span>) and 2016 (Day et al., <span>2016</span>). Previous versions of the guidelines have been cited in the peer-reviewed scientific literature several hundred times and downloaded from publishers' websites tens of thousands of times. The present document is an updated version of the guidelines. The VGG recognises that, given its ambition to produce guidelines with global applicability, its recommendations must be broad and based on fundamental immunological principles. Detailed recommendations about vaccines and vaccination of dogs and cats that might be suitable for some regions may be much less applicable elsewhere. In some countries where excellent national or regional vaccination guidelines have already been published these WSAVA guidelines may be less pertinent than what is already available. For example, guidelines have been authored for Israeli veterinarians that deal with vaccination of both dogs (Harrus, <span>2020</span>) and cats (Baneth, <span>2020</span>) in that country. Guidelines for the vaccination of dogs are available for Sri Lankan veterinary practitioners (Silva, <span>2016</span>). The American Animal Hospital Association (AAHA) and the American Association of Feline Practitioners (AAFP) have produced feline vaccination guidelines particularly relevant to North America (Stone et al., <span>2020</span>). AAHA has also produced canine vaccination guidelines particularly relevant to North America (Ellis et al., <span>2022</span>). The Advisory Board on Cat Diseases (ABCD) has produced feline vaccination guidelines most pertinent to Europe (ABCD, <span>2020a</span>, <span>2020b</span>, <span>2022</span>; Hosie et al., <span>2015</span>).</p><p>A key feature of these and other guidelines is the categorisation of vaccines as core, non-core or not recommended. In this latest version of the guidelines, the definition of core vaccines has been adjusted slightly to avoid self-contradictions and to improve clarity. This has also resulted in recategorisation of some vaccines. <i>Core vaccines</i> are those that ALL dogs and cats should receive, after considering their lifestyle and the geographical locations where they live or to which they travel. Core vaccines for dogs <i>in all countries of the world</i> are those that protect against CDV, CAV and CPV variants. Core vaccines for cats in all countries of the world are those that protect against FPV, FCV and FHV. For both cats and dogs, rabies virus vaccines should be considered core in all countries or regions where the disease is endemic.</p><p>Leptospirosis in dogs is another life-threatening, zoonotic disease that is widely distributed around the world. Vaccines to protect dogs against leptospirosis were categorised as non-core in previous versions of these guidelines. In countries or regions where canine leptospirosis occurs, where implicated serogroups are known and where suitable vaccines are available, vaccination of all dogs against leptospirosis is highly recommended and the vaccines should be considered core in those places. Feline leukaemia virus (FeLV) remains an important cause of morbidity and mortality in cats in many but not all parts of the world. In places where FeLV is prevalent or remains of concern, FeLV vaccines should be considered core in cats less than 1 year of age and in adult cats that have outdoor access or live with other cats that have outdoor access.</p><p><i>Non-core vaccines</i> are highly recommended only for those animals whose geographical location and/or lifestyle (<i>e.g</i>. indoor-outdoor access, multi-pet household) place them at risk of contracting specific infections not designated as core. <i>Not recommended vaccines</i> are those for which there is insufficient scientific evidence to justify recommending their use anywhere.</p><p>The basic structure of this latest revision of the guidelines is similar to that in the most recent previous version (Day et al., <span>2016</span>). However, this document has been extensively updated and includes numerous new reference citations.</p><p>These guidelines are intended to provide national small animal veterinary associations, veterinary practices and individual veterinarians with broad, up-to-date, scientifically supported advice about vaccination of dogs and cats. They offer strong advice in some areas but are not a set of rules. It would be impossible to produce a useful set of guiding rules that could apply to the more than 100 member associations in as many countries, and to the more than 200,000 individual veterinarians who comprise WSAVA. Across the WSAVA member associations, there are vast differences between countries and geographical regions in terms of infectious disease prevalence, how much is known about disease prevalence, vaccine products available, size of owned <i>versus</i> free-roaming dog and cat populations, practice and client economics and societal attitudes towards pets. A vaccine known by veterinarians to be crucially important in one country or region might justifiably be considered unhelpful and unnecessary elsewhere. Alternatively, it might simply be unavailable. It is up to national associations, local academic leaders and individual veterinarians to read, discuss and adapt these broad guidelines, in the context of local infectious disease prevalence and other factors, for their own member veterinarians and practices. In some countries and regions, this has already been done in recent years.</p><p>Practitioners are sometimes concerned that some guidelines recommendations run contrary to information in the product leaflet or datasheet (termed the “Summary of Product Characteristics” [SPC] in Europe). Some therefore worry that if they adopt guidelines recommendations, for example if they revaccinate adult animals less frequently than suggested in the product leaflet, or if they give additional doses of vaccine to animals between 12 and 20 weeks of age, they may leave themselves open to serious criticism. This is not generally the case (Thiry & Horzinek, <span>2007</span>); however, practitioners should ensure they remain up to date about any local or national regulations that may impede them from following guidelines. If such regulations run contrary to guidelines based on current scientific evidence and understanding, local or national veterinary organisations could consider lobbying authorities with the aim of having the regulations amended.</p><p>The product leaflet/data sheet/SPC is a legal document that forms part of the registration package for a vaccine. This document provides details about the safety and efficacy of the product and states the <i>minimum</i> DOI that can be expected after proper vaccination. Guidelines are based on all available evidence about DOI induced by vaccines for dogs and cats, not just on the minimum DOI data generated by manufacturers. Guidelines may therefore recommend triennial or less frequent revaccination with core vaccine products that may still carry a 1-year DOI claim in some countries. Although guidelines advice sometimes differs from information in the product leaflet, veterinarians can generally use a vaccine according to guidelines (and therefore current scientific thinking) by obtaining informed owner consent for this deviation from product leaflet recommendations (“off-label use”). Documentation of the informed consent in the medical record is advisable. A possible, rare exception would be countries where veterinarians might be compelled by government regulations to comply with label recommendations. Knowledge of any local regulations limiting veterinarians' freedom to deviate from product leaflet instructions is therefore important. Veterinarians should also bear in mind that company representatives will generally continue to advise that the veterinarian adheres to the instructions provided in their leaflets. They are required to do this, sometimes by law, even if they would prefer to support guidelines' recommendations.</p><p>These guidelines are based on published, peer-reviewed evidence wherever possible, but also, unavoidably, on unpublished or non-peer-reviewed scientific evidence and on expert opinions. Given the remarkable breadth of material to be covered in a single document, a narrative review format has once again been adopted as the only one suitable to the task (Baethge et al., <span>2019</span>). The same format has been chosen by all other international companion animal vaccination guidelines authoring teams (Ellis et al., <span>2022</span>; Hosie et al., <span>2015</span>; Stone et al., <span>2020</span>). Use of a systematic review format or a formal, structured approach to reach consensus recommendations based on the Delphi process, was considered by the VGG when planning this update (Gattrell et al., <span>2022</span>). These approaches were quickly deemed inapplicable given the breadth of material intended to be covered in a single document and the size of the authoring team. Nevertheless, these recommendations are based on the strongest scientific evidence that was found.</p><p>Regular assessment of vaccination needs is just one component of a comprehensive lifetime health care plan. Individualised patient care requires regular (usually annual) health checks, with the preventative health care plan designed around the age, breed, lifestyle, environment and travel activities of the pet and owner. Discussion of vaccination is one important part of such a visit, alongside consideration of ecto- and endoparasite detection, treatment and prevention, vector-borne and zoonotic disease prevention, dental care, nutritional advice, behavioural assessment and advice, and the necessity for any more frequent, tailored examinations of the pet.</p><p>In adult animals, decisions about revaccination with some of the core products (protecting against CDV, CAV and CPV in dogs and FPV in cats) can be informed by serological testing (Burr, <span>2006</span>). Some practitioners who offer this alternative to vaccination report that it is greatly appreciated by some owners (Killey et al., <span>2018</span>). This will be discussed in more detail in a later section.</p><p>There is little evidence that aged dogs and cats that have been vaccinated according to these guidelines throughout life require a specialised or enhanced programme of core revaccination late in life (Day, <span>2010</span>; Horzinek, <span>2010</span>; Schultz et al., <span>2010</span>). There is evidence that most aged dogs and cats have persisting immunological memory to core MLV vaccines (Dall'Ara et al., <span>2023</span>; Day, <span>2010</span>; HogenEsch et al., <span>2004</span>; Schultz et al., <span>2010</span>), with defence rapidly regained after administration of a single vaccine dose (Mouzin et al., <span>2004a</span>, <span>2004b</span>). By contrast, aged animals may not be so effective at mounting <i>primary</i> immune responses to novel agents or antigens that they have not previously encountered (Day, <span>2010</span>). In one recent study (Dall'Ara et al., <span>2023</span>) geriatric dogs vaccinated >3 years earlier were less likely to have protective antibody titres against CDV and CAV than geriatric dogs vaccinated 1 to 3 years earlier. Serological responses of these geriatric dogs to revaccination were not studied. Nevertheless, on the basis of these findings, revaccination of aged pets triennially or perhaps more frequently can be recommended.</p><p>Studies of UK dogs and cats vaccinated for the first time against rabies for pet travel have shown clearly that many aged animals fail to achieve the legally required antibody titre (Kennedy et al., <span>2007</span>; Mansfield et al., <span>2004</span>). Younger animals were more likely to be successfully immunised.</p><p>New kinds of vaccine have been developed and marketed since the last WSAVA vaccination guidelines were published (Day et al., <span>2016</span>). However, globally, the well-established vaccine types remain predominant and important, especially modified live and inactivated kinds.</p><p><i>Modified live or live attenuated vaccines</i> contain live but attenuated (<i>i.e</i>. weakened) whole viruses or bacterial organisms that can attach to cells, infect them and replicate within them, establishing a low-level and transient infection that engenders a strong immune response, without causing overt disease. Modified live vaccines are generally more immunogenic than most other kinds. Many MLV vaccines are particularly potent. They typically require fewer doses to achieve a strong immune response. Some modified live vaccines generate a consistent and long-lasting immune response (for many years) after a single dose, when administered to an animal in the absence of MDA interference. MLV vaccines have the advantage of more effectively inducing immunity at relevant anatomical sites when administered parenterally (usually subcutaneously) and are more likely than most other kinds to induce robust cellular as well as humoral (antibody-mediated) immunity. Some modified live vaccines are administered directly to mucosal sites (<i>e.g</i>. intranasal or oral vaccines) where they induce local, protective mucosal immunity.</p><p><i>Inactivated (or killed) vaccines</i> contain entire, inactivated, antigenically complete microorganisms that are not able to infect or replicate, but are able to stimulate an immune response. As they do not mimic a natural infection, they usually produce less potent immune responses, may not produce adequate mucosal or cellular immunity, and generally require multiple doses and an adjuvant to stimulate an adequate immune response. However, some inactivated vaccines are unusually potent, for example killed rabies virus vaccines. Some of these are highly immunogenic and can induce long-lasting protection after a single dose. Seroconversion of kittens after a single dose of inactivated vaccine has also been shown for FHV and FPV vaccines in kittens (Lappin, <span>2012</span>). In a subsequent FHV challenge study (Summers et al., <span>2017</span>), an inactivated vaccine provided similar protection to a MLV vaccine after challenge on day 7 after vaccination.</p><p>However, most inactivated vaccines are thought to require at least two initial doses to immunise, regardless of the animal's age. The first dose generally primes the immune response and the second (and sometimes a third) dose, usually administered 2 to 4 weeks apart, provides the protective immune response. A full protective immune response may not develop until 2 weeks after the second or final dose is given. Inactivated vaccines usually engender a shorter DOI when compared to MLV vaccines, and more frequent revaccination (<i>i.e</i>. boosting) is needed to maintain protection.</p><p><i>Subunit vaccines</i> consist of antigenic sub-components of pathogenic microorganisms that have been extracted and purified from cultures or have been synthesised using recombinant DNA technology (<i>i.e</i>. gene splicing and protein expression). These vaccines tend to be less immunogenic than MLV vaccines, so usually contain an adjuvant and engender a shorter DOI, like most inactivated vaccines. There are subunit vaccines for Lyme disease (Eschner & Mugnai, <span>2015</span>; Grosenbaugh et al., <span>2018</span>) and more recently for <i>Bordetella bronchiseptica</i> (containing fimbrial antigens), marketed for use in dogs (HPRA, <span>2024</span>; MSD Animal Health, <span>2024</span>).</p><p>Recombinant DNA technology has recently been used to produce a <i>novel live recombinant vaccine</i> against CPV (Pearce et al., <span>2023</span>). The novel CPV component is combined with a more conventional MLV CDV component (European Medicines Agency, <span>2021</span>). This vaccine is intended to protect puppies against CPV infection at a very young age (4 weeks) by breaking through MDA interference more effectively than previous generation vaccines. This vaccine contains a recombinant, chimaeric parvoviral genome, part CPV-2c and part CPV-2. During manufacture, the recombinant genome is used to produce live parvovirus that can infect cells and multiply in vaccinated puppies, just like a conventionally manufactured live attenuated vaccine.</p><p><i>Vectored vaccines</i> are another kind of recombinant vaccine, in which one or more genes that encode immunogenic proteins of one or more pathogens are cloned directly into the genome of a vector virus or organism (<i>e.g</i>. an attenuated canarypoxvirus vector with the rabies virus surface glycoprotein gene spliced into place). This avian recombinant, chimaeric virus can replicate only to a very limited extent in the mammalian host but does express the introduced gene(s) on host cell surfaces, mimicking a natural infection. Vectored vaccines cannot revert to virulence and the vector is chosen to be non-pathogenic and sometimes immunostimulatory. These vaccines can induce both humoral and cellular immune responses, usually without the need for an adjuvant. Attenuated canarypoxvirus has been used in vectored vaccines against rabies, canine distemper and FeLV infection.</p><p><i>Nucleic acid-based vaccines</i> (DNA and RNA vaccines) are relatively new forms of vaccine created by manipulating nucleic acids to produce copies of viral antigenic target proteins upon immunisation. Messenger RNA (mRNA) vaccines have become familiar to many people during the current COVID-19 pandemic. They generally require very cold transportation and storage. Messenger RNA vaccines employ delivery systems, such as lipid nanoparticles, that protect the nucleic acid from degradation and that allow cellular uptake and mRNA release. DNA is much less fragile than mRNA, so naked DNA vaccines are more robust. There are currently no mRNA vaccines, nor naked DNA vaccines, available for use in dogs and cats.</p><p>MDA are mostly acquired by neonatal puppies and kittens by consuming colostrum in the first hours after they are born (Chastant & Mila, <span>2019</span>; Rossi et al., <span>2021</span>). MDA provides passive immunity. Although important to protect puppies and kittens in the first weeks of life, MDA can also interfere with the ability of the young animal to mount its own, active immune response to most vaccines (DiGangi, Levy, et al., <span>2011b</span>; Friedrich & Truyen, <span>2000</span>). Serum MDA inhibits immunoglobulin G (IgG) production within the young animal and prevents vaccine antigens from stimulating an active immune response. In most puppies and kittens, MDA declines to levels that allow an active immune response to vaccination by about 8 to 12 weeks of age. Puppies with low amounts of MDA may be vulnerable (and capable of responding to vaccination) at an earlier age, while others may possess MDA at such high levels that they are incapable of responding to vaccination until ≥12 weeks of age (Friedrich & Truyen, <span>2000</span>; Thibault et al., <span>2016</span>). The period when MDA is insufficient to provide complete immunologic protection, but still enough to interfere with an active immune response, is known as the “window of susceptibility” for the puppy or kitten. During this “window,” a puppy or kitten cannot be immunised by conventional vaccines but is susceptible to disease if it comes into contact with “street” or virulent pathogen. It is not possible, without serological testing, to predict when this “window” will open or close (<i>i.e</i>. begin or end) because the amount of MDA transferred to individual puppies or kittens varies between litters and within litters. As it is impossible to predict, without blood testing, when sufficient waning of MDA will occur, the initial core vaccination series usually involves the administration of multiple, sequential doses. The repeated doses are not booster doses. They are applied with the aim of triggering an active immune response as soon as possible after MDA has dropped sufficiently (see Fig 1). MDA can interfere with immune responses to both modified live and inactivated vaccines. If, when administering the first dose of an inactivated vaccine, there is enough MDA to block an active immune response, immune priming will not occur. A second dose of inactivated vaccine would then fail to immunise the animal. Conversely, a single dose of MLV vaccine given after MDA has waned sufficiently is usually sufficient to immunise.</p><p>An advance in companion animal practice is the commercial availability of in-practice diagnostic test kits that can detect antibodies against CDV, CPV and CAV in dogs and FPV in cats. Some of these test kits have been validated for use in practice and shelter settings and are simple to use (Egerer et al., <span>2022</span>; Gray et al., <span>2012</span>; Litster et al., <span>2012</span>; Meazzi et al., <span>2022</span>). They provide a rapid result (positive or negative) within 20 to 30 minutes. Some of these test kits may usefully complement traditional laboratory-based methods (<i>e.g</i>. virus neutralisation and haemagglutination inhibition testing), which remain the “gold standards” for serological testing (Jenkins et al., <span>2020</span>).</p><p>For CDV, CPV and CAV in adult dogs and FPV in adult cats, the presence of serum antibody provides evidence of an active humoral immune response, which is very likely to indicate protection from disease. In some pets, these antibodies persist for well over 3 years. Vaccinated dogs may maintain protective immunity against CDV, CPV and CAV for many years (Bohm et al., <span>2004</span>; Jensen et al., <span>2015</span>; Mitchell et al., <span>2012</span>; Mouzin et al., <span>2004a</span>, <span>2004b</span>; Schultz, <span>2006</span>; Schultz et al., <span>2010</span>). The same is true of FPV in cats.</p><p>Conversely, the presence of antibody against FHV or FCV is currently not considered to be a reliable predictor of immune protection against either of these viruses (Egberink et al., <span>2022</span>; Stone et al., <span>2020</span>) although an earlier study did provide supportive results in shelter cats (DiGangi et al., <span>2011a</span>). Vaccines intended to protect against FHV and FCV cause seroconversion but may only provide partial protection against disease and do not protect effectively against infection or development of the carrier state. In cats, tests for anti-FPV antibodies are considered more reliable indicators of protection than tests that detect anti-FHV and anti-FCV antibodies (Mende et al., <span>2014</span>).</p><p>As opposed to the presence of antibody, the <i>absence</i> of detectable antibody does not reliably predict susceptibility to infection and disease. This is because cellular and innate immunity are not evaluated in antibody detection testing and many animals are thought to be robustly protected by immunological memory in the absence of detectable serum antibody (Killey et al., <span>2018</span>). In support of this, prompt, strong anamnestic antibody responses have been demonstrated in previously vaccinated, seronegative pet animals shortly after revaccination, indicating that they would likely have been robustly protected from challenge (Mitchell et al., <span>2012</span>; Mouzin et al., <span>2004a</span>, <span>2004b</span>). Despite these findings, absence of antibodies has generally been taken as a clinical indication for revaccination. This is based on a precautionary principle because proof of memory (other than retrospectively by revaccination and retesting) cannot readily be achieved in most clinical settings.</p><p>An owner may wish to confirm that a puppy or kitten has mounted an active immune response after the course of primary vaccinations has finished. If so, a serum sample taken at or after 20 weeks of age and at least 4 weeks after the last vaccine dose can be tested. Animals discovered to be seronegative (probably only a small percentage) should be revaccinated and retested several weeks later. If the animal again tests negative, it should tentatively be considered a non-responder that may be incapable of developing protective immunity against the pathogen(s) for which it tests seronegative. Performing a gold standard serological test at this stage may refute the earlier in-practice results or show a low or undetectable antibody titre typical of a non-responder dog (see Fig 2).</p><p>In-practice serological test kits have gained favour with some veterinarians who wish to offer their clients a convenient alternative to routine revaccination at (for example) 3-yearly intervals. However, in-practice serological test kits have been shown to vary in sensitivity, specificity, positive and negative predictive value (PPV and NPV), and overall accuracy (OA) when compared to reference, gold standard tests (Bergmann et al., <span>2020</span>; Bergmann, Halzheu, et al., <span>2021a</span>; Bergmann, Zablotski, et al., <span>2021b</span>; Dall'Ara et al., <span>2021</span>; DiGangi, Gray, et al., <span>2011a</span>; Egerer et al., <span>2022</span>; Meazzi et al., <span>2022</span>; Mende et al., <span>2014</span>).</p><p>The specificity of in-practice serological test kits needs to be high if they are to be relied upon (Bergmann et al., <span>2020</span>; Bergmann, Halzheu, et al., <span>2021a</span>; Bergmann, Zablotski, et al., <span>2021b</span>). A false positive result would suggest that an animal has antibodies and is protected. In fact, because the result is a <i>false</i> positive, current guidelines recommend that the animal should be revaccinated. Recently, several different in-practice diagnostic test kits were compared with gold standard testing in Germany (Bergmann et al., <span>2020</span>; Bergmann, Halzheu, et al., <span>2021a</span>; Bergmann, Zablotski, et al., <span>2021b</span>). The kits varied in ease-of-use and in performance relative to the gold standard tests. Some of the tested kits performed very well for detection of CPV-2 antibody in canine serum (Bergmann et al., <span>2020</span>) but kits for detection of CDV antibody, and a kit for detection of CAV antibody, performed much less well (Bergmann, Halzheu, et al., <span>2021a</span>; Bergmann, Zablotski, et al., <span>2021b</span>). Four different in-practice kits for detection of CDV antibody were compared to a gold standard. Against the gold standard, they were not reliable when used to test dogs with acute illness or healthy-looking dogs with chronic disease (Bergmann, Zablotski, et al., <span>2021b</span>). The reliability of the gold standard virus neutralisation test for CDV, when used in acutely ill or chronically diseased dogs, was also questioned in this paper. Overall, the usefulness of in-practice serological testing for detection of anti-CDV antibody using these test kits, certainly in acutely ill dogs or in dogs with chronic disease, was not supported by this work (Bergmann, Zablotski, et al., <span>2021b</span>). A single test kit for detection of anti-CAV antibodies had poor specificity (Bergmann, Holzheu, et al., <span>2021a</span>). Further research is needed to boost progress in this important area.</p><p>Understanding the utility and limitations of serological testing as an aid to vaccination-related decision-making is demanding. Veterinarians should not feel obliged to start using serological or “titre” testing in their practices, if they are not inclined to do so. Several FAQs dealing with serological testing have been included in this latest version of the guidelines. These are for those veterinarians who may be interested in exploring this topic further.</p><p>Most of the contemporary issues discussed in the 2016 version of these guidelines (Day et al., <span>2016</span>) remain of current interest although many further topics and issues have emerged since then. Since 2016, concerns about a low proportion of all pets receiving the benefit of vaccination have grown in some countries (Malter et al., <span>2022</span>; Taylor et al., <span>2022</span>). A low proportion of vaccinated pet animals adversely impacts “herd immunity” (Datta & Roy, <span>2022</span>). The concept of herd immunity needs to be understood and acted upon by companion animal veterinarians. Frequent revaccination of a small proportion of pets within a population will do little to improve herd immunity. Conversely, increasing the proportion of vaccinated pets within the population, even if each of those pets receives only a single, well-timed core vaccine, will achieve far more.</p><p>Excessive, unwarranted “vaccine load” remains of concern and, indeed, the situation has deteriorated in some countries. Multi-component vaccines that contain a mixture of core and non-core components remain common. In at least one country, monovalent vaccine choices have diminished rather than expanding, as would be preferable.</p><p>The concept of “One Health” has never been more pertinent to companion animal practice than it is today. The suffering of humans and the suffering of their companion cats and dogs have been interwoven during the COVID-19 pandemic (Baptista et al., <span>2020</span>). Just as the pandemic delayed elective surgical and medical procedures in countless humans, it prevented pet owners from obtaining timely veterinary care, especially vaccinations, for their pets (Owczarczak-Garstecka et al., <span>2022</span>). Thankfully, that situation has improved in many countries since the beginning of the pandemic. There have been many other One Health implications of COVID-19. A renewed global focus on pandemic preparedness is an opportunity for the One Health initiative, since many potential human pathogens either have animal reservoirs or equivalent animal pathogens. Further, new vaccine platform technologies used for human pathogens may catalyse innovative veterinary vaccine development.</p><p>“Vaccination hesitancy” is another issue of considerable contemporary importance. Concerns about worsening vaccine hesitancy have been expressed by members of both veterinary and medical organisations (Lee et al., <span>2022</span>; Mattson, <span>2020</span>). Vaccine or vaccination hesitancy has been described as a “…<i>delay in acceptance or refusal of vaccination despite availability of vaccination services</i>.” (MacDonald, <span>2015</span>). Vaccine hesitancy is of enormous and growing concern to public health authorities around the world, including the World Health Organization (WHO). Indeed, in 2019, vaccine hesitancy was listed as one of the top 10 threats to global human health (WHO, <span>2019</span>). The phrase “vaccine hesitancy” first appeared in the Web of Science Core Collection in 2010. Since then, use of the phrase has increased substantially with more than 350 papers on this topic published in 2020 alone (Squires, <span>2021a</span>). The description provided above is not sufficiently inclusive for small companion animal practitioners. This is because many people who choose not to vaccinate their pets do so without ever consulting a veterinarian. They do not delay acceptance, nor refuse, they simply avoid any discussion (Squires, <span>2021b</span>).</p><p>There are scant data on vaccine hesitancy in small companion animal practice, but over 2500 veterinary practitioners in numerous countries responded in an informal survey and the results indicated that it is perceived by many veterinarians as a growing problem (Squires, <span>2021b</span>). In support of this, data about many aspects of companion animal welfare collected in the United Kingdom from 2011 to 2022 (PDSA, <span>2022</span>) began to reveal an alarming decline (first noticed in 2017) in the proportion of UK pets reported by owners as being vaccinated. In the PDSA's 2019 PAW Report only 72% of owners reported that their puppy had received a primary course of vaccines (down from about 88% in 2016). The figure was lower for kittens: 61%, down from about 82% in 2016. The proportion of adult dogs and cats receiving regular booster revaccinations was even lower. In 2020 to 2022 (PDSA, <span>2022</span>), the situation seemed to stabilise or improve, with slightly larger proportions of animals receiving vaccines, but the confounding effects of the COVID-19 pandemic make it difficult to interpret these more recently reported figures.</p><p>In the 2019 PAW report, <i>“It's too expensive”</i> was a top reason for not having vaccination done (17% of all pet owners). For owners of adult cats, not wanting to stress the cat by taking it to the veterinary clinic was a powerful inhibitor to seeking revaccination, slightly more powerful than cost (influencing 22% of owners <i>versus</i> 21% influenced by cost). Thus, Fear Free Pets® and other similar organisations may be able to play important roles in improving compliance with vaccination recommendations. Interestingly, concern about vaccine safety was not mentioned as a reason for failure to vaccinate pet dogs or cats in the 2019 PAW report.</p><p>In a recent study of almost 1 million UK dogs, Taylor et al. (<span>2022</span>) showed that only 49% had received at least one vaccine against leptospirosis in the 12-month study period. In this study, Dogs over 8 years of age were 12.5 times less likely to have received the benefit of vaccination against leptospirosis than were dogs under 1 year of age.</p><p>Another recent study looked at variability in non-core vaccination rates of dogs and cats in veterinary clinics across the USA (Malter et al., <span>2022</span>). These animals were all up to date for their core vaccines. Nationally, in this study, median clinic vaccination rates for dogs were 70.5% for leptospirosis and 68.7% for <i>Bordetella bronchiseptica</i>. In cats, for FeLV, median clinic vaccination rates were reportedly low for adult cats (34.6%) and only slightly higher for kittens and 1-year-old cats (36.8%).</p><p>Clearly, there remains considerable scope for veterinarians and veterinary associations to work to improve small companion animal vaccination rates, including in some rather wealthy countries.</p><p>Regarding excessive “vaccine load” it is disappointing that, for example in Australia, it is no longer possible to purchase a monovalent FeLV vaccine. The situation has deteriorated since the last iteration of these guidelines. The only option now is to inject a pentavalent, inactivated vaccine that includes FeLV. Previously there were several monovalent choices. Presumably, commercial imperatives in a relatively small market have led to this situation.</p><p>There are two basic types of shelter for housing homeless animals: <i>traditional shelters</i> that provide temporary housing pending placement into homes and <i>sanctuaries</i> where animals remain for life. The traditional shelter population has a higher turnover rate and short periods of residence with constant arrival and departure of animals. Sanctuaries have more stable populations based on long-term residence and low turnover. The average population in either type of shelter can range from a few dozen to hundreds of animals. Both types admit animals from random sources in the community, most of which have no prior veterinary care, substantially increasing the risk for introduction and spread of contagious diseases and establishment of endemic disease.</p><p>The high risk for disease exposure in shelters requires a robust vaccination programme that not only protects each animal but the population as a whole. What best serves individual animals in lower exposure risk home environments is not ideal for the high-risk shelter environment. According to the Association of Shelter Veterinarians' Guidelines for Standards of Care in Animal Shelters, 2nd Edition (The Association of Shelter Veterinarians, <span>2022</span>) “<i>Shelter vaccine protocols differ from protocols used in private practice because shelter animals are subject to an increased risk of infectious disease… Key differences in [shelter vaccine] protocols compared to those recommended in private practice include an earlier and longer age range for juveniles, a shorter time span between vaccines, and different core and noncore products</i>.”</p><p>CDV, CPV and FPV commonly cause life-threatening illness in dogs and cats in shelters. Every shelter is a high-risk environment for exposure to these pathogens and most have been affected by costly outbreaks in terms of animal suffering and death. While CDV, CPV and FPV infections cause highest mortality, contagious respiratory infections are the most frequently occurring form of illness in shelters. <i>B. bronchiseptica</i>, CAV-2, CPiV and CDV are prevalent respiratory pathogens in shelter dogs (Day et al., <span>2020</span>; Lavan & Knesl, <span>2015</span>; Monteiro et al., <span>2016</span>; Schulz et al., <span>2014</span>; Sowman et al., <span>2018</span>). FHV and FCV are the most prevalent respiratory pathogens detected in shelter cats (Bannasch & Foley, <span>2005</span>; McManus et al., <span>2014</span>).</p><p>Most puppies and kittens less than 6 months old, and 30% to 50% of adult dogs and cats, have little or no detectable antibody to CDV, CPV, FPV, FHV and FCV on admission into shelters in the USA (DiGangi et al., <span>2012</span>; Fischer et al., <span>2007</span>; Lechner et al., <span>2010</span>; Litster et al., <span>2012</span>). This indicates that many animals enter shelters with inadequate protection against the most common diseases. For this reason, early immunisation of as many individuals as possible is paramount to disease control in shelters. The cornerstone is vaccination of <i>all dogs and cats immediately upon admission</i>. A delay of even 1 day can significantly increase the risk for infection and spread of disease within the population (Bannasch & Foley, <span>2005</span>). Delays in vaccination have greater consequences for animals in shelters than in typical homes.</p><p>Adverse events are detrimental, unintended consequences that follow vaccine administration (including lack of protection). They include any hypersensitivity reaction, illness, injury, or apparent toxic effect. Local reactions such as pain and swelling at the injection site and systemic reactions such as lethargy, anorexia, fever and vomiting are commonly observed (Miyaji et al., <span>2012</span>; Moore et al., <span>2005</span>, <span>2007</span>; Yoshida et al., <span>2021</span>, <span>2022</span>). Urticaria and anaphylaxis are less common (Tizard, <span>2021</span>). AEFVs should be reported <i>even when their association with vaccination is only suspected</i>. Each vaccine adverse event report should identify the implicated vaccine product (including batch number), details of the animal involved, details of the adverse event and contact details of the veterinarian submitting the report.</p><p>Veterinarian-reported field observations of suspected AEFVs are the most important way that manufacturers and regulatory authorities can be alerted to potential vaccine safety or efficacy problems. Pre-licensure safety studies will only detect relatively common adverse events. Rarer adverse events are detected through post-marketing surveillance and analysis of reported adverse events. Reports should be sent to the manufacturer and to the local regulatory authority. In some countries government surveillance schemes do not yet exist and therefore AEFVs can only be reported to the manufacturer. The VGG recognises that there is gross under-reporting of AEFVs. This impedes growth of knowledge about the safety and efficacy of vaccine products. The VGG actively encourages all veterinarians to participate vigorously in reporting suspected vaccine-associated adverse events.</p><p>Lack of expected efficacy of a vaccine is an adverse event. As explained previously, a very common cause in young animals is interference caused by maternally transferred colostral antibodies. However, there are other important causes. Poor vaccine husbandry, a surprisingly common problem, may be responsible. Practices should consider nominating specific staff members to be responsible for overseeing, monitoring and reporting upon vaccine husbandry. Vaccines that are batch-reconstituted and left to stand for hours before being drawn up and injected may lose potency. This particularly affects the more fragile vaccine components, such as CDV. Vaccines placed in the refrigerator too close to the freezer compartment may freeze, losing potency. Old refrigerators are especially prone to this and may also have defective seals, so that vaccines are not stored at a sufficiently low temperature (generally 2 to 8°C). Use of multidose vials (<i>e.g</i>. 10 rabies vaccine doses in a single vial) may be associated with lack of efficacy if a vaccine suspension is not adequately mixed before each and every dose is drawn up. This may also cause overdosing of some recipients, increasing the probability of other kinds of adverse event, such as hypersensitivity reactions or pain at the time of injection and post-vaccinal swellings.</p><p>Given the unique, enormous, almost 100-fold, variation in size and bodyweight of adult domestic dogs, it is interesting that vaccine manufacturers continue to recommend that adult dogs of all sizes receive the same dose of vaccine (Tizard, <span>2021</span>). In addition, for most vaccines, the dose supplied for young puppies is identical to what is supplied for much larger and more mature adults. Conversely, for humans, it was recently decided that smaller doses of COVID-19 vaccine should be supplied for young children as compared with adults. Geriatric adults receive higher doses of influenza vaccines.</p><p>Provision of identical doses to dogs of all sizes and ages remains current, standard practice, and the VGG is <i>not</i> encouraging veterinarians to deviate from manufacturers' advice in this regard. However, it is noteworthy that small dogs are the ones more prone to experience post-vaccinal adverse events (Moore et al., <span>2005</span>; Yao et al., <span>2015</span>). The adverse reaction rate also increased as more, separate vaccines were given at the same visit. Large and giant dogs are less likely to mount a sufficient immune response to rabies vaccination than are small dogs (Jakel et al., <span>2008</span>; Tizard, <span>2021</span>). In one study, bodyweight was inversely correlated with the magnitude of anti-CPV and anti-CDV antibody responses; that is, small dogs mounted stronger antibody responses than did large and giant ones, although adequate, protective responses were produced by dogs of all sizes (Taguchi et al., <span>2012</span>). Recent work done in the USA on a very large population of dogs (nearly 5 million) has shown that breed appears to be a determinant of the likelihood of AEFVs, independent of bodyweight (Moore et al., <span>2023</span>). Some breeds of dog have a much higher risk of experiencing acute AEFVs than does the general population. French Bulldogs, Dachshunds and Boston terriers, were at highest risk. Small dogs (<5 kg bodyweight) that received multiple vaccines per visit were at particular risk. More research is needed into appropriate vaccine doses for individual dogs, given the enormous size and breed variations among domestic dogs.</p><p>In future, the definition of AEFVs may be broadened to include more explicitly some rare, potential or actual adverse health consequences of pet vaccination for immunocompromised <i>owners</i>. For example, mucosally administered modified live bacterial vaccines (such as some of the <i>B. bronchiseptica</i> vaccines) have recently been suggested to represent a health hazard for some humans, including those with cystic fibrosis (Moore, Rendall & Millar, <span>2022</span>). Although the risk appears small, it has been suggested that it might be prudent to ask immunocompromised client pet owners to leave the consulting room while modified live <i>B. bronchiseptica</i> mucosal vaccines are being administered (Weese, <span>2021</span>). This begs the question: how would the veterinarian know which clients to ask to leave the room? Questioning clients about their immunological health is not yet common practice in companion animal medicine (although occasionally clients volunteer this sort of information). Use of subunit or inactivated <i>B. bronchiseptica</i> vaccines would presumably be safer for immunocompromised pet owners, assuming equivalent protection is provided by these vaccines (Ellis, <span>2015</span>).</p>","PeriodicalId":17062,"journal":{"name":"Journal of Small Animal Practice","volume":"65 5","pages":"277-316"},"PeriodicalIF":1.9000,"publicationDate":"2024-04-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jsap.13718","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Small Animal Practice","FirstCategoryId":"97","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jsap.13718","RegionNum":2,"RegionCategory":"农林科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"VETERINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
The World Small Animal Veterinary Association (WSAVA) Vaccination Guidelines Group (VGG) was convened to develop guidelines for the vaccination of dogs and cats intended to be helpful to veterinarians globally. Previous guidelines, published in 2007, 2010 and 2016, have been cited in the peer-reviewed scientific literature several hundred times and downloaded tens of thousands of times. The present document is an updated version of these guidelines. The VGG recognises that its recommendations must be broad and based on fundamental immunological principles because detailed recommendations about vaccines and vaccination of dogs and cats that might be suitable for some countries or regions may be much less applicable elsewhere.
Guidelines are intended to provide broad guidance for veterinarians in decision-making. They do not describe mandatory or minimum standards of care. These guidelines can be used by national and regional veterinary associations and individual veterinarians or veterinary practices to develop their own vaccination schedules suitable to their own local conditions. Notwithstanding this, the VGG strongly recommends that ALL dogs and cats should receive the benefit of vaccination. This will not only protect individual animals but will improve “herd immunity” to help minimise the risk of contagious disease outbreaks.
With this background in mind, the VGG has defined core vaccines as those that ALL dogs and cats should receive, after considering their lifestyle and the geographical areas in which they live or to which they travel. Some core vaccines protect animals from potentially life-threatening diseases that have global distribution while others protect against life-threatening diseases that are prevalent only in particular countries or regions. Core vaccines for dogs in all parts of the world are those that protect against canine distemper virus (CDV), canine adenovirus type 1 (CAV) and canine parvovirus type 2 (CPV). Core vaccines for cats in all parts of the world are those that protect against feline parvovirus (FPV), feline calicivirus (FCV) and feline herpesvirus-1 (FHV). In areas of the world where rabies is endemic, vaccination against rabies virus should be considered essential for both dogs and cats (i.e. rabies vaccines are core in those places), even if there is no legal requirement for this. Leptospirosis in dogs is another life-threatening, zoonotic disease that is widely distributed around the world. In countries or regions where canine leptospirosis is endemic, where implicated serogroups are known and where suitable vaccines are available, vaccination of all dogs against leptospirosis is highly recommended and the vaccines should be considered core in those places. In many parts of the world, feline leukaemia virus (FeLV)-related diseases are endemic. In these places, FeLV vaccines should be considered core for young cats (<1 year of age) and for adult cats with outdoor access or that live with other cats that have outdoor access.
The VGG recognises that maternally derived antibodies (MDAs) interfere substantially with the efficacy of most currently available core vaccines that are administered to puppies and kittens early in life (protecting against CDV, CAV and CPV in puppies, FPV, FCV and FHV in kittens). As the level of MDA varies substantially within and between litters, VGG recommends the administration of multiple core vaccine doses to puppies and kittens, every 2 to 4 weeks, with the final dose being delivered at 16 weeks of age or older. In situations where a puppy or kitten can only receive a single vaccination (e.g. in the case of cost constraints), vaccination should be with the core vaccines at 16+ weeks of age. Revaccination at or after 26 weeks of age (rather than waiting until 12 to 16 months of age) is advised to immunise without unnecessary delay the minority of animals that may still have had interfering MDA present at the time of their 16+ week vaccination.
The VGG supports the use of serological testing from 20 weeks of age onwards to detect seroconversion (to CDV, CAV and CPV in dogs and FPV in cats) following vaccination. This can help confirm active immune protection in young and young adult animals, help optimise revaccination intervals in mature adult animals, and in some situations, can help in the management of contagious disease outbreaks in shelters.
Vaccines should not be given needlessly. Core vaccines should not be given any more frequently than necessary in adult animals. There is an abundance of peer-reviewed, published evidence showing that the duration of immunity (DOI) provided by most, modern, modified live virus (MLV) core vaccines is many years.
The VGG has defined non-core vaccines as those that should be highly recommended in animals whose geographical location and/or lifestyle (e.g. indoor-outdoor access, multi-pet household) places them at risk of contracting particular infections not designated as core. A careful conversation between veterinarian and owner is needed to inform the decision about which non-core vaccines to recommend for each patient. The VGG has classified some vaccines as not recommended where there is insufficient scientific evidence to justify recommending their use anywhere. The VGG has not considered a few “minor” vaccine products that have very restricted geographical availability or applicability.
The VGG strongly encourages veterinarians to educate their clients about the value of regular health checks (usually annual, sometimes more often) as opposed to speaking of “vaccination consultations.” The annual health check is much more than just a vaccination consultation, although it will often include administration of selected vaccines that need to be administered annually. The DOI provided by most non-core vaccines is about 1 year.
Veterinarians are also encouraged to undergo training intended to improve the experience of pets, owners and veterinary staff before and during pet health check visits. The Free Fear training programme (https://fearfreepets.com/fear-free-certification-overview/) and the Cat Friendly Certificate programme (https://catvets.com/cfp/cat-friendly-certificate-program/) are examples.
The VGG has considered the use of vaccines in shelters and sanctuaries, again recognising the financial constraints under which some of these facilities operate. The VGG minimum shelter guidelines state that all dogs and cats entering such establishments should be vaccinated before, or at the time of their entry, with the core MLV vaccines. Where finances permit, these vaccines should be administered every 2 to 3 weeks starting at 4 weeks of age and continuing until 5 months of age. Vaccines against respiratory disease are considered non-core for pet dogs living in typical homes but should be considered core for shelter-housed dogs.
The VGG recognises the importance of adverse reaction reporting schemes but understands that these are variably developed in different countries. Veterinarians are strongly encouraged to report all possible adverse events to the manufacturer and to the regulatory authority to expand the knowledge base that drives development of improved, safer vaccines.
The WSAVA VGG was convened in 2006 to develop guidelines for the vaccination of dogs and cats intended to be helpful to veterinarians globally. Previous guidelines were published in 2007 (Day, Horzinek & Schultz 2007a), 2010 (Day et al., 2010) and 2016 (Day et al., 2016). Previous versions of the guidelines have been cited in the peer-reviewed scientific literature several hundred times and downloaded from publishers' websites tens of thousands of times. The present document is an updated version of the guidelines. The VGG recognises that, given its ambition to produce guidelines with global applicability, its recommendations must be broad and based on fundamental immunological principles. Detailed recommendations about vaccines and vaccination of dogs and cats that might be suitable for some regions may be much less applicable elsewhere. In some countries where excellent national or regional vaccination guidelines have already been published these WSAVA guidelines may be less pertinent than what is already available. For example, guidelines have been authored for Israeli veterinarians that deal with vaccination of both dogs (Harrus, 2020) and cats (Baneth, 2020) in that country. Guidelines for the vaccination of dogs are available for Sri Lankan veterinary practitioners (Silva, 2016). The American Animal Hospital Association (AAHA) and the American Association of Feline Practitioners (AAFP) have produced feline vaccination guidelines particularly relevant to North America (Stone et al., 2020). AAHA has also produced canine vaccination guidelines particularly relevant to North America (Ellis et al., 2022). The Advisory Board on Cat Diseases (ABCD) has produced feline vaccination guidelines most pertinent to Europe (ABCD, 2020a, 2020b, 2022; Hosie et al., 2015).
A key feature of these and other guidelines is the categorisation of vaccines as core, non-core or not recommended. In this latest version of the guidelines, the definition of core vaccines has been adjusted slightly to avoid self-contradictions and to improve clarity. This has also resulted in recategorisation of some vaccines. Core vaccines are those that ALL dogs and cats should receive, after considering their lifestyle and the geographical locations where they live or to which they travel. Core vaccines for dogs in all countries of the world are those that protect against CDV, CAV and CPV variants. Core vaccines for cats in all countries of the world are those that protect against FPV, FCV and FHV. For both cats and dogs, rabies virus vaccines should be considered core in all countries or regions where the disease is endemic.
Leptospirosis in dogs is another life-threatening, zoonotic disease that is widely distributed around the world. Vaccines to protect dogs against leptospirosis were categorised as non-core in previous versions of these guidelines. In countries or regions where canine leptospirosis occurs, where implicated serogroups are known and where suitable vaccines are available, vaccination of all dogs against leptospirosis is highly recommended and the vaccines should be considered core in those places. Feline leukaemia virus (FeLV) remains an important cause of morbidity and mortality in cats in many but not all parts of the world. In places where FeLV is prevalent or remains of concern, FeLV vaccines should be considered core in cats less than 1 year of age and in adult cats that have outdoor access or live with other cats that have outdoor access.
Non-core vaccines are highly recommended only for those animals whose geographical location and/or lifestyle (e.g. indoor-outdoor access, multi-pet household) place them at risk of contracting specific infections not designated as core. Not recommended vaccines are those for which there is insufficient scientific evidence to justify recommending their use anywhere.
The basic structure of this latest revision of the guidelines is similar to that in the most recent previous version (Day et al., 2016). However, this document has been extensively updated and includes numerous new reference citations.
These guidelines are intended to provide national small animal veterinary associations, veterinary practices and individual veterinarians with broad, up-to-date, scientifically supported advice about vaccination of dogs and cats. They offer strong advice in some areas but are not a set of rules. It would be impossible to produce a useful set of guiding rules that could apply to the more than 100 member associations in as many countries, and to the more than 200,000 individual veterinarians who comprise WSAVA. Across the WSAVA member associations, there are vast differences between countries and geographical regions in terms of infectious disease prevalence, how much is known about disease prevalence, vaccine products available, size of owned versus free-roaming dog and cat populations, practice and client economics and societal attitudes towards pets. A vaccine known by veterinarians to be crucially important in one country or region might justifiably be considered unhelpful and unnecessary elsewhere. Alternatively, it might simply be unavailable. It is up to national associations, local academic leaders and individual veterinarians to read, discuss and adapt these broad guidelines, in the context of local infectious disease prevalence and other factors, for their own member veterinarians and practices. In some countries and regions, this has already been done in recent years.
Practitioners are sometimes concerned that some guidelines recommendations run contrary to information in the product leaflet or datasheet (termed the “Summary of Product Characteristics” [SPC] in Europe). Some therefore worry that if they adopt guidelines recommendations, for example if they revaccinate adult animals less frequently than suggested in the product leaflet, or if they give additional doses of vaccine to animals between 12 and 20 weeks of age, they may leave themselves open to serious criticism. This is not generally the case (Thiry & Horzinek, 2007); however, practitioners should ensure they remain up to date about any local or national regulations that may impede them from following guidelines. If such regulations run contrary to guidelines based on current scientific evidence and understanding, local or national veterinary organisations could consider lobbying authorities with the aim of having the regulations amended.
The product leaflet/data sheet/SPC is a legal document that forms part of the registration package for a vaccine. This document provides details about the safety and efficacy of the product and states the minimum DOI that can be expected after proper vaccination. Guidelines are based on all available evidence about DOI induced by vaccines for dogs and cats, not just on the minimum DOI data generated by manufacturers. Guidelines may therefore recommend triennial or less frequent revaccination with core vaccine products that may still carry a 1-year DOI claim in some countries. Although guidelines advice sometimes differs from information in the product leaflet, veterinarians can generally use a vaccine according to guidelines (and therefore current scientific thinking) by obtaining informed owner consent for this deviation from product leaflet recommendations (“off-label use”). Documentation of the informed consent in the medical record is advisable. A possible, rare exception would be countries where veterinarians might be compelled by government regulations to comply with label recommendations. Knowledge of any local regulations limiting veterinarians' freedom to deviate from product leaflet instructions is therefore important. Veterinarians should also bear in mind that company representatives will generally continue to advise that the veterinarian adheres to the instructions provided in their leaflets. They are required to do this, sometimes by law, even if they would prefer to support guidelines' recommendations.
These guidelines are based on published, peer-reviewed evidence wherever possible, but also, unavoidably, on unpublished or non-peer-reviewed scientific evidence and on expert opinions. Given the remarkable breadth of material to be covered in a single document, a narrative review format has once again been adopted as the only one suitable to the task (Baethge et al., 2019). The same format has been chosen by all other international companion animal vaccination guidelines authoring teams (Ellis et al., 2022; Hosie et al., 2015; Stone et al., 2020). Use of a systematic review format or a formal, structured approach to reach consensus recommendations based on the Delphi process, was considered by the VGG when planning this update (Gattrell et al., 2022). These approaches were quickly deemed inapplicable given the breadth of material intended to be covered in a single document and the size of the authoring team. Nevertheless, these recommendations are based on the strongest scientific evidence that was found.
Regular assessment of vaccination needs is just one component of a comprehensive lifetime health care plan. Individualised patient care requires regular (usually annual) health checks, with the preventative health care plan designed around the age, breed, lifestyle, environment and travel activities of the pet and owner. Discussion of vaccination is one important part of such a visit, alongside consideration of ecto- and endoparasite detection, treatment and prevention, vector-borne and zoonotic disease prevention, dental care, nutritional advice, behavioural assessment and advice, and the necessity for any more frequent, tailored examinations of the pet.
In adult animals, decisions about revaccination with some of the core products (protecting against CDV, CAV and CPV in dogs and FPV in cats) can be informed by serological testing (Burr, 2006). Some practitioners who offer this alternative to vaccination report that it is greatly appreciated by some owners (Killey et al., 2018). This will be discussed in more detail in a later section.
There is little evidence that aged dogs and cats that have been vaccinated according to these guidelines throughout life require a specialised or enhanced programme of core revaccination late in life (Day, 2010; Horzinek, 2010; Schultz et al., 2010). There is evidence that most aged dogs and cats have persisting immunological memory to core MLV vaccines (Dall'Ara et al., 2023; Day, 2010; HogenEsch et al., 2004; Schultz et al., 2010), with defence rapidly regained after administration of a single vaccine dose (Mouzin et al., 2004a, 2004b). By contrast, aged animals may not be so effective at mounting primary immune responses to novel agents or antigens that they have not previously encountered (Day, 2010). In one recent study (Dall'Ara et al., 2023) geriatric dogs vaccinated >3 years earlier were less likely to have protective antibody titres against CDV and CAV than geriatric dogs vaccinated 1 to 3 years earlier. Serological responses of these geriatric dogs to revaccination were not studied. Nevertheless, on the basis of these findings, revaccination of aged pets triennially or perhaps more frequently can be recommended.
Studies of UK dogs and cats vaccinated for the first time against rabies for pet travel have shown clearly that many aged animals fail to achieve the legally required antibody titre (Kennedy et al., 2007; Mansfield et al., 2004). Younger animals were more likely to be successfully immunised.
New kinds of vaccine have been developed and marketed since the last WSAVA vaccination guidelines were published (Day et al., 2016). However, globally, the well-established vaccine types remain predominant and important, especially modified live and inactivated kinds.
Modified live or live attenuated vaccines contain live but attenuated (i.e. weakened) whole viruses or bacterial organisms that can attach to cells, infect them and replicate within them, establishing a low-level and transient infection that engenders a strong immune response, without causing overt disease. Modified live vaccines are generally more immunogenic than most other kinds. Many MLV vaccines are particularly potent. They typically require fewer doses to achieve a strong immune response. Some modified live vaccines generate a consistent and long-lasting immune response (for many years) after a single dose, when administered to an animal in the absence of MDA interference. MLV vaccines have the advantage of more effectively inducing immunity at relevant anatomical sites when administered parenterally (usually subcutaneously) and are more likely than most other kinds to induce robust cellular as well as humoral (antibody-mediated) immunity. Some modified live vaccines are administered directly to mucosal sites (e.g. intranasal or oral vaccines) where they induce local, protective mucosal immunity.
Inactivated (or killed) vaccines contain entire, inactivated, antigenically complete microorganisms that are not able to infect or replicate, but are able to stimulate an immune response. As they do not mimic a natural infection, they usually produce less potent immune responses, may not produce adequate mucosal or cellular immunity, and generally require multiple doses and an adjuvant to stimulate an adequate immune response. However, some inactivated vaccines are unusually potent, for example killed rabies virus vaccines. Some of these are highly immunogenic and can induce long-lasting protection after a single dose. Seroconversion of kittens after a single dose of inactivated vaccine has also been shown for FHV and FPV vaccines in kittens (Lappin, 2012). In a subsequent FHV challenge study (Summers et al., 2017), an inactivated vaccine provided similar protection to a MLV vaccine after challenge on day 7 after vaccination.
However, most inactivated vaccines are thought to require at least two initial doses to immunise, regardless of the animal's age. The first dose generally primes the immune response and the second (and sometimes a third) dose, usually administered 2 to 4 weeks apart, provides the protective immune response. A full protective immune response may not develop until 2 weeks after the second or final dose is given. Inactivated vaccines usually engender a shorter DOI when compared to MLV vaccines, and more frequent revaccination (i.e. boosting) is needed to maintain protection.
Subunit vaccines consist of antigenic sub-components of pathogenic microorganisms that have been extracted and purified from cultures or have been synthesised using recombinant DNA technology (i.e. gene splicing and protein expression). These vaccines tend to be less immunogenic than MLV vaccines, so usually contain an adjuvant and engender a shorter DOI, like most inactivated vaccines. There are subunit vaccines for Lyme disease (Eschner & Mugnai, 2015; Grosenbaugh et al., 2018) and more recently for Bordetella bronchiseptica (containing fimbrial antigens), marketed for use in dogs (HPRA, 2024; MSD Animal Health, 2024).
Recombinant DNA technology has recently been used to produce a novel live recombinant vaccine against CPV (Pearce et al., 2023). The novel CPV component is combined with a more conventional MLV CDV component (European Medicines Agency, 2021). This vaccine is intended to protect puppies against CPV infection at a very young age (4 weeks) by breaking through MDA interference more effectively than previous generation vaccines. This vaccine contains a recombinant, chimaeric parvoviral genome, part CPV-2c and part CPV-2. During manufacture, the recombinant genome is used to produce live parvovirus that can infect cells and multiply in vaccinated puppies, just like a conventionally manufactured live attenuated vaccine.
Vectored vaccines are another kind of recombinant vaccine, in which one or more genes that encode immunogenic proteins of one or more pathogens are cloned directly into the genome of a vector virus or organism (e.g. an attenuated canarypoxvirus vector with the rabies virus surface glycoprotein gene spliced into place). This avian recombinant, chimaeric virus can replicate only to a very limited extent in the mammalian host but does express the introduced gene(s) on host cell surfaces, mimicking a natural infection. Vectored vaccines cannot revert to virulence and the vector is chosen to be non-pathogenic and sometimes immunostimulatory. These vaccines can induce both humoral and cellular immune responses, usually without the need for an adjuvant. Attenuated canarypoxvirus has been used in vectored vaccines against rabies, canine distemper and FeLV infection.
Nucleic acid-based vaccines (DNA and RNA vaccines) are relatively new forms of vaccine created by manipulating nucleic acids to produce copies of viral antigenic target proteins upon immunisation. Messenger RNA (mRNA) vaccines have become familiar to many people during the current COVID-19 pandemic. They generally require very cold transportation and storage. Messenger RNA vaccines employ delivery systems, such as lipid nanoparticles, that protect the nucleic acid from degradation and that allow cellular uptake and mRNA release. DNA is much less fragile than mRNA, so naked DNA vaccines are more robust. There are currently no mRNA vaccines, nor naked DNA vaccines, available for use in dogs and cats.
MDA are mostly acquired by neonatal puppies and kittens by consuming colostrum in the first hours after they are born (Chastant & Mila, 2019; Rossi et al., 2021). MDA provides passive immunity. Although important to protect puppies and kittens in the first weeks of life, MDA can also interfere with the ability of the young animal to mount its own, active immune response to most vaccines (DiGangi, Levy, et al., 2011b; Friedrich & Truyen, 2000). Serum MDA inhibits immunoglobulin G (IgG) production within the young animal and prevents vaccine antigens from stimulating an active immune response. In most puppies and kittens, MDA declines to levels that allow an active immune response to vaccination by about 8 to 12 weeks of age. Puppies with low amounts of MDA may be vulnerable (and capable of responding to vaccination) at an earlier age, while others may possess MDA at such high levels that they are incapable of responding to vaccination until ≥12 weeks of age (Friedrich & Truyen, 2000; Thibault et al., 2016). The period when MDA is insufficient to provide complete immunologic protection, but still enough to interfere with an active immune response, is known as the “window of susceptibility” for the puppy or kitten. During this “window,” a puppy or kitten cannot be immunised by conventional vaccines but is susceptible to disease if it comes into contact with “street” or virulent pathogen. It is not possible, without serological testing, to predict when this “window” will open or close (i.e. begin or end) because the amount of MDA transferred to individual puppies or kittens varies between litters and within litters. As it is impossible to predict, without blood testing, when sufficient waning of MDA will occur, the initial core vaccination series usually involves the administration of multiple, sequential doses. The repeated doses are not booster doses. They are applied with the aim of triggering an active immune response as soon as possible after MDA has dropped sufficiently (see Fig 1). MDA can interfere with immune responses to both modified live and inactivated vaccines. If, when administering the first dose of an inactivated vaccine, there is enough MDA to block an active immune response, immune priming will not occur. A second dose of inactivated vaccine would then fail to immunise the animal. Conversely, a single dose of MLV vaccine given after MDA has waned sufficiently is usually sufficient to immunise.
An advance in companion animal practice is the commercial availability of in-practice diagnostic test kits that can detect antibodies against CDV, CPV and CAV in dogs and FPV in cats. Some of these test kits have been validated for use in practice and shelter settings and are simple to use (Egerer et al., 2022; Gray et al., 2012; Litster et al., 2012; Meazzi et al., 2022). They provide a rapid result (positive or negative) within 20 to 30 minutes. Some of these test kits may usefully complement traditional laboratory-based methods (e.g. virus neutralisation and haemagglutination inhibition testing), which remain the “gold standards” for serological testing (Jenkins et al., 2020).
For CDV, CPV and CAV in adult dogs and FPV in adult cats, the presence of serum antibody provides evidence of an active humoral immune response, which is very likely to indicate protection from disease. In some pets, these antibodies persist for well over 3 years. Vaccinated dogs may maintain protective immunity against CDV, CPV and CAV for many years (Bohm et al., 2004; Jensen et al., 2015; Mitchell et al., 2012; Mouzin et al., 2004a, 2004b; Schultz, 2006; Schultz et al., 2010). The same is true of FPV in cats.
Conversely, the presence of antibody against FHV or FCV is currently not considered to be a reliable predictor of immune protection against either of these viruses (Egberink et al., 2022; Stone et al., 2020) although an earlier study did provide supportive results in shelter cats (DiGangi et al., 2011a). Vaccines intended to protect against FHV and FCV cause seroconversion but may only provide partial protection against disease and do not protect effectively against infection or development of the carrier state. In cats, tests for anti-FPV antibodies are considered more reliable indicators of protection than tests that detect anti-FHV and anti-FCV antibodies (Mende et al., 2014).
As opposed to the presence of antibody, the absence of detectable antibody does not reliably predict susceptibility to infection and disease. This is because cellular and innate immunity are not evaluated in antibody detection testing and many animals are thought to be robustly protected by immunological memory in the absence of detectable serum antibody (Killey et al., 2018). In support of this, prompt, strong anamnestic antibody responses have been demonstrated in previously vaccinated, seronegative pet animals shortly after revaccination, indicating that they would likely have been robustly protected from challenge (Mitchell et al., 2012; Mouzin et al., 2004a, 2004b). Despite these findings, absence of antibodies has generally been taken as a clinical indication for revaccination. This is based on a precautionary principle because proof of memory (other than retrospectively by revaccination and retesting) cannot readily be achieved in most clinical settings.
An owner may wish to confirm that a puppy or kitten has mounted an active immune response after the course of primary vaccinations has finished. If so, a serum sample taken at or after 20 weeks of age and at least 4 weeks after the last vaccine dose can be tested. Animals discovered to be seronegative (probably only a small percentage) should be revaccinated and retested several weeks later. If the animal again tests negative, it should tentatively be considered a non-responder that may be incapable of developing protective immunity against the pathogen(s) for which it tests seronegative. Performing a gold standard serological test at this stage may refute the earlier in-practice results or show a low or undetectable antibody titre typical of a non-responder dog (see Fig 2).
In-practice serological test kits have gained favour with some veterinarians who wish to offer their clients a convenient alternative to routine revaccination at (for example) 3-yearly intervals. However, in-practice serological test kits have been shown to vary in sensitivity, specificity, positive and negative predictive value (PPV and NPV), and overall accuracy (OA) when compared to reference, gold standard tests (Bergmann et al., 2020; Bergmann, Halzheu, et al., 2021a; Bergmann, Zablotski, et al., 2021b; Dall'Ara et al., 2021; DiGangi, Gray, et al., 2011a; Egerer et al., 2022; Meazzi et al., 2022; Mende et al., 2014).
The specificity of in-practice serological test kits needs to be high if they are to be relied upon (Bergmann et al., 2020; Bergmann, Halzheu, et al., 2021a; Bergmann, Zablotski, et al., 2021b). A false positive result would suggest that an animal has antibodies and is protected. In fact, because the result is a false positive, current guidelines recommend that the animal should be revaccinated. Recently, several different in-practice diagnostic test kits were compared with gold standard testing in Germany (Bergmann et al., 2020; Bergmann, Halzheu, et al., 2021a; Bergmann, Zablotski, et al., 2021b). The kits varied in ease-of-use and in performance relative to the gold standard tests. Some of the tested kits performed very well for detection of CPV-2 antibody in canine serum (Bergmann et al., 2020) but kits for detection of CDV antibody, and a kit for detection of CAV antibody, performed much less well (Bergmann, Halzheu, et al., 2021a; Bergmann, Zablotski, et al., 2021b). Four different in-practice kits for detection of CDV antibody were compared to a gold standard. Against the gold standard, they were not reliable when used to test dogs with acute illness or healthy-looking dogs with chronic disease (Bergmann, Zablotski, et al., 2021b). The reliability of the gold standard virus neutralisation test for CDV, when used in acutely ill or chronically diseased dogs, was also questioned in this paper. Overall, the usefulness of in-practice serological testing for detection of anti-CDV antibody using these test kits, certainly in acutely ill dogs or in dogs with chronic disease, was not supported by this work (Bergmann, Zablotski, et al., 2021b). A single test kit for detection of anti-CAV antibodies had poor specificity (Bergmann, Holzheu, et al., 2021a). Further research is needed to boost progress in this important area.
Understanding the utility and limitations of serological testing as an aid to vaccination-related decision-making is demanding. Veterinarians should not feel obliged to start using serological or “titre” testing in their practices, if they are not inclined to do so. Several FAQs dealing with serological testing have been included in this latest version of the guidelines. These are for those veterinarians who may be interested in exploring this topic further.
Most of the contemporary issues discussed in the 2016 version of these guidelines (Day et al., 2016) remain of current interest although many further topics and issues have emerged since then. Since 2016, concerns about a low proportion of all pets receiving the benefit of vaccination have grown in some countries (Malter et al., 2022; Taylor et al., 2022). A low proportion of vaccinated pet animals adversely impacts “herd immunity” (Datta & Roy, 2022). The concept of herd immunity needs to be understood and acted upon by companion animal veterinarians. Frequent revaccination of a small proportion of pets within a population will do little to improve herd immunity. Conversely, increasing the proportion of vaccinated pets within the population, even if each of those pets receives only a single, well-timed core vaccine, will achieve far more.
Excessive, unwarranted “vaccine load” remains of concern and, indeed, the situation has deteriorated in some countries. Multi-component vaccines that contain a mixture of core and non-core components remain common. In at least one country, monovalent vaccine choices have diminished rather than expanding, as would be preferable.
The concept of “One Health” has never been more pertinent to companion animal practice than it is today. The suffering of humans and the suffering of their companion cats and dogs have been interwoven during the COVID-19 pandemic (Baptista et al., 2020). Just as the pandemic delayed elective surgical and medical procedures in countless humans, it prevented pet owners from obtaining timely veterinary care, especially vaccinations, for their pets (Owczarczak-Garstecka et al., 2022). Thankfully, that situation has improved in many countries since the beginning of the pandemic. There have been many other One Health implications of COVID-19. A renewed global focus on pandemic preparedness is an opportunity for the One Health initiative, since many potential human pathogens either have animal reservoirs or equivalent animal pathogens. Further, new vaccine platform technologies used for human pathogens may catalyse innovative veterinary vaccine development.
“Vaccination hesitancy” is another issue of considerable contemporary importance. Concerns about worsening vaccine hesitancy have been expressed by members of both veterinary and medical organisations (Lee et al., 2022; Mattson, 2020). Vaccine or vaccination hesitancy has been described as a “…delay in acceptance or refusal of vaccination despite availability of vaccination services.” (MacDonald, 2015). Vaccine hesitancy is of enormous and growing concern to public health authorities around the world, including the World Health Organization (WHO). Indeed, in 2019, vaccine hesitancy was listed as one of the top 10 threats to global human health (WHO, 2019). The phrase “vaccine hesitancy” first appeared in the Web of Science Core Collection in 2010. Since then, use of the phrase has increased substantially with more than 350 papers on this topic published in 2020 alone (Squires, 2021a). The description provided above is not sufficiently inclusive for small companion animal practitioners. This is because many people who choose not to vaccinate their pets do so without ever consulting a veterinarian. They do not delay acceptance, nor refuse, they simply avoid any discussion (Squires, 2021b).
There are scant data on vaccine hesitancy in small companion animal practice, but over 2500 veterinary practitioners in numerous countries responded in an informal survey and the results indicated that it is perceived by many veterinarians as a growing problem (Squires, 2021b). In support of this, data about many aspects of companion animal welfare collected in the United Kingdom from 2011 to 2022 (PDSA, 2022) began to reveal an alarming decline (first noticed in 2017) in the proportion of UK pets reported by owners as being vaccinated. In the PDSA's 2019 PAW Report only 72% of owners reported that their puppy had received a primary course of vaccines (down from about 88% in 2016). The figure was lower for kittens: 61%, down from about 82% in 2016. The proportion of adult dogs and cats receiving regular booster revaccinations was even lower. In 2020 to 2022 (PDSA, 2022), the situation seemed to stabilise or improve, with slightly larger proportions of animals receiving vaccines, but the confounding effects of the COVID-19 pandemic make it difficult to interpret these more recently reported figures.
In the 2019 PAW report, “It's too expensive” was a top reason for not having vaccination done (17% of all pet owners). For owners of adult cats, not wanting to stress the cat by taking it to the veterinary clinic was a powerful inhibitor to seeking revaccination, slightly more powerful than cost (influencing 22% of owners versus 21% influenced by cost). Thus, Fear Free Pets® and other similar organisations may be able to play important roles in improving compliance with vaccination recommendations. Interestingly, concern about vaccine safety was not mentioned as a reason for failure to vaccinate pet dogs or cats in the 2019 PAW report.
In a recent study of almost 1 million UK dogs, Taylor et al. (2022) showed that only 49% had received at least one vaccine against leptospirosis in the 12-month study period. In this study, Dogs over 8 years of age were 12.5 times less likely to have received the benefit of vaccination against leptospirosis than were dogs under 1 year of age.
Another recent study looked at variability in non-core vaccination rates of dogs and cats in veterinary clinics across the USA (Malter et al., 2022). These animals were all up to date for their core vaccines. Nationally, in this study, median clinic vaccination rates for dogs were 70.5% for leptospirosis and 68.7% for Bordetella bronchiseptica. In cats, for FeLV, median clinic vaccination rates were reportedly low for adult cats (34.6%) and only slightly higher for kittens and 1-year-old cats (36.8%).
Clearly, there remains considerable scope for veterinarians and veterinary associations to work to improve small companion animal vaccination rates, including in some rather wealthy countries.
Regarding excessive “vaccine load” it is disappointing that, for example in Australia, it is no longer possible to purchase a monovalent FeLV vaccine. The situation has deteriorated since the last iteration of these guidelines. The only option now is to inject a pentavalent, inactivated vaccine that includes FeLV. Previously there were several monovalent choices. Presumably, commercial imperatives in a relatively small market have led to this situation.
There are two basic types of shelter for housing homeless animals: traditional shelters that provide temporary housing pending placement into homes and sanctuaries where animals remain for life. The traditional shelter population has a higher turnover rate and short periods of residence with constant arrival and departure of animals. Sanctuaries have more stable populations based on long-term residence and low turnover. The average population in either type of shelter can range from a few dozen to hundreds of animals. Both types admit animals from random sources in the community, most of which have no prior veterinary care, substantially increasing the risk for introduction and spread of contagious diseases and establishment of endemic disease.
The high risk for disease exposure in shelters requires a robust vaccination programme that not only protects each animal but the population as a whole. What best serves individual animals in lower exposure risk home environments is not ideal for the high-risk shelter environment. According to the Association of Shelter Veterinarians' Guidelines for Standards of Care in Animal Shelters, 2nd Edition (The Association of Shelter Veterinarians, 2022) “Shelter vaccine protocols differ from protocols used in private practice because shelter animals are subject to an increased risk of infectious disease… Key differences in [shelter vaccine] protocols compared to those recommended in private practice include an earlier and longer age range for juveniles, a shorter time span between vaccines, and different core and noncore products.”
CDV, CPV and FPV commonly cause life-threatening illness in dogs and cats in shelters. Every shelter is a high-risk environment for exposure to these pathogens and most have been affected by costly outbreaks in terms of animal suffering and death. While CDV, CPV and FPV infections cause highest mortality, contagious respiratory infections are the most frequently occurring form of illness in shelters. B. bronchiseptica, CAV-2, CPiV and CDV are prevalent respiratory pathogens in shelter dogs (Day et al., 2020; Lavan & Knesl, 2015; Monteiro et al., 2016; Schulz et al., 2014; Sowman et al., 2018). FHV and FCV are the most prevalent respiratory pathogens detected in shelter cats (Bannasch & Foley, 2005; McManus et al., 2014).
Most puppies and kittens less than 6 months old, and 30% to 50% of adult dogs and cats, have little or no detectable antibody to CDV, CPV, FPV, FHV and FCV on admission into shelters in the USA (DiGangi et al., 2012; Fischer et al., 2007; Lechner et al., 2010; Litster et al., 2012). This indicates that many animals enter shelters with inadequate protection against the most common diseases. For this reason, early immunisation of as many individuals as possible is paramount to disease control in shelters. The cornerstone is vaccination of all dogs and cats immediately upon admission. A delay of even 1 day can significantly increase the risk for infection and spread of disease within the population (Bannasch & Foley, 2005). Delays in vaccination have greater consequences for animals in shelters than in typical homes.
Adverse events are detrimental, unintended consequences that follow vaccine administration (including lack of protection). They include any hypersensitivity reaction, illness, injury, or apparent toxic effect. Local reactions such as pain and swelling at the injection site and systemic reactions such as lethargy, anorexia, fever and vomiting are commonly observed (Miyaji et al., 2012; Moore et al., 2005, 2007; Yoshida et al., 2021, 2022). Urticaria and anaphylaxis are less common (Tizard, 2021). AEFVs should be reported even when their association with vaccination is only suspected. Each vaccine adverse event report should identify the implicated vaccine product (including batch number), details of the animal involved, details of the adverse event and contact details of the veterinarian submitting the report.
Veterinarian-reported field observations of suspected AEFVs are the most important way that manufacturers and regulatory authorities can be alerted to potential vaccine safety or efficacy problems. Pre-licensure safety studies will only detect relatively common adverse events. Rarer adverse events are detected through post-marketing surveillance and analysis of reported adverse events. Reports should be sent to the manufacturer and to the local regulatory authority. In some countries government surveillance schemes do not yet exist and therefore AEFVs can only be reported to the manufacturer. The VGG recognises that there is gross under-reporting of AEFVs. This impedes growth of knowledge about the safety and efficacy of vaccine products. The VGG actively encourages all veterinarians to participate vigorously in reporting suspected vaccine-associated adverse events.
Lack of expected efficacy of a vaccine is an adverse event. As explained previously, a very common cause in young animals is interference caused by maternally transferred colostral antibodies. However, there are other important causes. Poor vaccine husbandry, a surprisingly common problem, may be responsible. Practices should consider nominating specific staff members to be responsible for overseeing, monitoring and reporting upon vaccine husbandry. Vaccines that are batch-reconstituted and left to stand for hours before being drawn up and injected may lose potency. This particularly affects the more fragile vaccine components, such as CDV. Vaccines placed in the refrigerator too close to the freezer compartment may freeze, losing potency. Old refrigerators are especially prone to this and may also have defective seals, so that vaccines are not stored at a sufficiently low temperature (generally 2 to 8°C). Use of multidose vials (e.g. 10 rabies vaccine doses in a single vial) may be associated with lack of efficacy if a vaccine suspension is not adequately mixed before each and every dose is drawn up. This may also cause overdosing of some recipients, increasing the probability of other kinds of adverse event, such as hypersensitivity reactions or pain at the time of injection and post-vaccinal swellings.
Given the unique, enormous, almost 100-fold, variation in size and bodyweight of adult domestic dogs, it is interesting that vaccine manufacturers continue to recommend that adult dogs of all sizes receive the same dose of vaccine (Tizard, 2021). In addition, for most vaccines, the dose supplied for young puppies is identical to what is supplied for much larger and more mature adults. Conversely, for humans, it was recently decided that smaller doses of COVID-19 vaccine should be supplied for young children as compared with adults. Geriatric adults receive higher doses of influenza vaccines.
Provision of identical doses to dogs of all sizes and ages remains current, standard practice, and the VGG is not encouraging veterinarians to deviate from manufacturers' advice in this regard. However, it is noteworthy that small dogs are the ones more prone to experience post-vaccinal adverse events (Moore et al., 2005; Yao et al., 2015). The adverse reaction rate also increased as more, separate vaccines were given at the same visit. Large and giant dogs are less likely to mount a sufficient immune response to rabies vaccination than are small dogs (Jakel et al., 2008; Tizard, 2021). In one study, bodyweight was inversely correlated with the magnitude of anti-CPV and anti-CDV antibody responses; that is, small dogs mounted stronger antibody responses than did large and giant ones, although adequate, protective responses were produced by dogs of all sizes (Taguchi et al., 2012). Recent work done in the USA on a very large population of dogs (nearly 5 million) has shown that breed appears to be a determinant of the likelihood of AEFVs, independent of bodyweight (Moore et al., 2023). Some breeds of dog have a much higher risk of experiencing acute AEFVs than does the general population. French Bulldogs, Dachshunds and Boston terriers, were at highest risk. Small dogs (<5 kg bodyweight) that received multiple vaccines per visit were at particular risk. More research is needed into appropriate vaccine doses for individual dogs, given the enormous size and breed variations among domestic dogs.
In future, the definition of AEFVs may be broadened to include more explicitly some rare, potential or actual adverse health consequences of pet vaccination for immunocompromised owners. For example, mucosally administered modified live bacterial vaccines (such as some of the B. bronchiseptica vaccines) have recently been suggested to represent a health hazard for some humans, including those with cystic fibrosis (Moore, Rendall & Millar, 2022). Although the risk appears small, it has been suggested that it might be prudent to ask immunocompromised client pet owners to leave the consulting room while modified live B. bronchiseptica mucosal vaccines are being administered (Weese, 2021). This begs the question: how would the veterinarian know which clients to ask to leave the room? Questioning clients about their immunological health is not yet common practice in companion animal medicine (although occasionally clients volunteer this sort of information). Use of subunit or inactivated B. bronchiseptica vaccines would presumably be safer for immunocompromised pet owners, assuming equivalent protection is provided by these vaccines (Ellis, 2015).
期刊介绍:
Journal of Small Animal Practice (JSAP) is a monthly peer-reviewed publication integrating clinical research papers and case reports from international sources, covering all aspects of medicine and surgery relating to dogs, cats and other small animals. These papers facilitate the dissemination and implementation of new ideas and techniques relating to clinical veterinary practice, with the ultimate aim of promoting best practice. JSAP publishes high quality original articles, as well as other scientific and educational information. New developments are placed in perspective, encompassing new concepts and peer commentary. The target audience is veterinarians primarily engaged in the practise of small animal medicine and surgery.
In addition to original articles, JSAP will publish invited editorials (relating to a manuscript in the same issue or a topic of current interest), review articles, which provide in-depth discussion of important clinical issues, and other scientific and educational information from around the world.
The final decision on publication of a manuscript rests with the Editorial Board and ultimately with the Editor. All papers, regardless of type, represent the opinion of the authors and not necessarily that of the Editor, the Association or the Publisher.
The Journal of Small Animal Practice is published on behalf of the British Small Animal Veterinary Association and is also the official scientific journal of the World Small Animal Veterinary Association
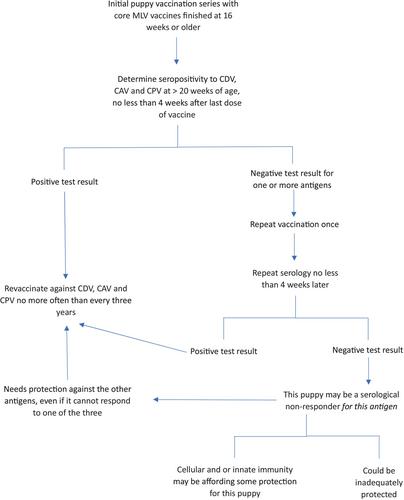




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
