Mariana Bastos-Oreiro, Pau Abrisqueta, Antonio Gutierrez, Ana Jiménez Ubieto, Maria Poza, Paula Fernanez-Caldas, María José LLacer, Sonia Gonzalez de Villambrosia, Raúl Córdoba, Alberto López, Elena Ceballos, Belen Navarro, Ana Muntañola, Eva Donato, Eva Diez-Baeza, Lourdes Escoda, Hugo Luzardo, María José Peñarrubia, Daniel García Belmonte, Emilia Pardal, Claudia Lozada, Alejandro Martín García-Sancho
{"title":"New therapies for relapsed or refractory aggressive B-cell lymphoma increase survival: Analysis from the RELINF registry of the GELTAMO group","authors":"Mariana Bastos-Oreiro, Pau Abrisqueta, Antonio Gutierrez, Ana Jiménez Ubieto, Maria Poza, Paula Fernanez-Caldas, María José LLacer, Sonia Gonzalez de Villambrosia, Raúl Córdoba, Alberto López, Elena Ceballos, Belen Navarro, Ana Muntañola, Eva Donato, Eva Diez-Baeza, Lourdes Escoda, Hugo Luzardo, María José Peñarrubia, Daniel García Belmonte, Emilia Pardal, Claudia Lozada, Alejandro Martín García-Sancho","doi":"10.1002/hem3.70","DOIUrl":null,"url":null,"abstract":"<p>Aggressive B-cell lymphomas (ABCL) represent a heterogeneous group of biologically different diseases with variable clinical outcomes.<span><sup>1, 2</sup></span> Around one-third of patients are not cured with frontline treatment, and outcomes for this relapse/refractory (R/R) group are extremely poor with conventional treatments.<span><sup>3-5</sup></span> However, during the last years, several promising new therapies (NTs) have been progressively incorporated into the treatment arsenal, such as new monoclonal antibodies (MAs), cellular therapy with T cells with chimeric antigen receptor (CAR-T cells), or, in a lesser extent, bispecific antibodies (BiMAs). Polatuzumab vedotin–bendamustine–rituximab<span><sup>6</sup></span> was approved in Europe since 2019 and funded in Spain since September 2019. Tafasitamab–lenalidomide<span><sup>7</sup></span> was approved for European Medicines Agency (EMA) in August 2021 and funded in Spain in 2023. CAR-T cell was approved for EMA in 2018,<span><sup>8-10</sup></span> and funded in Spain in 2019. BiMAs are still only available in clinical trials.<span><sup>11, 12</sup></span></p><p>Our study aims to assess to what extent these new treatments have been incorporated into the clinical practice and how this has impacted patient survival.</p><p>This is a multicentre retrospective study based on the GELTAMO RELINF platform, which has been active since January 2014 and includes only essential variables such as histological subtype, age, gender, and current situation. From 60 centers actively registering on the platform invited to participate, 17 centers accepted. All of these centers are university hospitals, and five are CAR-T cell therapy providers. Participating centers completed a short questionnaire on disease relapse and the use of NTs in their registered patients. Conventional treatments only include chemotherapy ± anti-CD20 antibodies ± autologous transplant. Investigators in each center were required to report relapses with histological confirmation of large B-cell lymphoma (LBCL). For refractory patients, histological confirmation was not mandatory. The histologies included were diffuse LBCL (DLBCL) and high-grade B-cell lymphoma (HGBCL) not otherwise specified (NOS) and double hit. Early relapse was defined as within 12 months of completion of induction therapy, and late relapse was defined as more than 12 months.</p><p>The present analysis was based on a January 2023 data cut-off. Overall survival (OS) and progression-free survival (PFS) were determined from diagnosis. OS was also calculated since the date of the first relapse (OS2). All reported <i>p</i> values were two-sided, and statistical significance was set at <i>p</i> < 0.05. Analyses were performed using SPSS version 29 (SPSS).</p><p>From 3270 patients with ABCL registered, 2853 patients were included in the present analysis; exclusion reasons are described in Supporting Information S1: Table 1.</p><p>Supporting Information S1: Table 2 shows patients' characteristics. Three hundred fifty-three patients (47.8%) were identified as primary refractory, whereas 139 patients (19%) relapsed between 3 months and 1 year after completion of induction treatment. These 492 patients were analyzed together as the “early relapse group” (67% of R/R patients). Two hundred and forty-six patients had a late relapse (33%). The distribution was 132 (54%) during the second year, 51 (21%) during the third year, 24 (10%) during the fourth, 16 (6%) during the fifth year, and 23 (10%) from the sixth year onward.</p><p>Supporting Information S1: Table 3 describes the characteristics and outcomes of patients who relapsed early and late. A third of relapses were in patients older than 80 years. Regarding histologies, early relapses were most common in double/triple hit HGL (34%) and T-cell rich DLBCL (29%) compared to DLBCL or HGL NOS (16%) (<i>p</i> < 0.001).</p><p>Of 738 patients with detailed information on the type of salvage treatments, 236 received NT: 144 received CAR-T (90 as the only NT), 68 BiMAs (27 as the only NT), 92 polatuzumab-based (46 as the only TN), 14 tafasitamab–lenalidomide (12 as the only NT), and 61 received multiple NTs. Specific information on the number of treatment lines was available in 730 of the 738 patients. The median number of lines among R/R patients was 2.<span><sup>1-10</sup></span> The use of NT was much more frequent in patients who received three or more lines of treatment. The immense majority of patients who received only two treatment lines (<i>n</i> = 376) were treated with conventional treatments (90%), and only 38 (10%) received NT. By contrast, among 354 patients who received more than two lines of treatment, 194 (55%) received NT: 130 (67%) received CAR-T cell therapy (80 as the only NT), 75 (21%) polatuzumab (35 as the only NT), nine (2%) tafasitamab–lenalidomide (seven as the only NT), 55 (15%) BiMA (18 as the only NT), 54 (30%) received multiple NTs, whereas 160 (45%) of these patients did not receive any NT. While 175 (74%) patients received just one NT, 50 (21%) received two combined NTs, and 11 (5%) received three. As shown in Supporting Information S1: Table 4, there were no differences in the timing of relapse (early vs. late) between patients treated with conventional treatments versus NT.</p><p>With a median follow-up of 49 months (95% confidence interval, CI: 47–51), the median PFS for the entire cohort was 54 months (95% CI: 48–61), and the median OS was 82 months (95% CI: 74–90) (Supporting Information S1: Figure 1A).</p><p>Supporting Information S1: Table 5 shows factors identified as related to OS, since diagnosis. In multivariate analysis, early relapse (hazard ratio, HR 2.91 [95% CI: 2.35–3.6]; <i>p</i> < 0.001), number of total lines (HR 1.4 [95% CI: 1.14–1.71]; <i>p</i> = 0.018), age over 65 years (HR 1.83 [95% CI: 1.17–2.86]; <i>p</i> = 0.008), age over 75 years (HR 2.86 [95% CI: 1.84–4.46]; <i>p</i> < 0.001), use of CAR-T cell therapy (HR 0.67 [95% CI: 0.47–0.96]; <i>p</i> = 0.029), and BiMAs (HR 0.5 [95% CI: 0.37–0.68]; <i>p</i> < 0.001) impacted on OS.</p><p>Considering the 738 R/R patients only, with a median follow-up of 40 months, the median OS (mOS2) was 16.8 (95% CI: 14.5–19) months (Supporting Information S1: Figure 1B). It was longer for the group of patients treated with more than two lines (19 months [95% CI: 16–22]) than in patients treated with only two lines (11 months [95% CI: 6–17]; <i>p</i> < 0.001) (Figure 1A).</p><p>Median OS2 was significantly shorter (<i>p</i> < 0.001) in the early relapse group (13.5 months [95% CI: 11.5–15.5]) than in late relapses (31.1 months [95% CI: 22.5–39.8]; <i>p</i> < 0.001) (Figure 1B). Median OS2 for relapsed patients treated with NT was 31.1 months (95% CI: 22.5–39.7) compared with 11.9 months (95% CI: 9.2–14.6) for the group of standard treatment (<i>p</i> < 0.001) (Figure 1C). Patients who received CAR-T cell therapy had better OS2 than those who did not (<i>p</i> < 0.001) (Figure 1D). Among early relapses, the median OS2 for patients who received CAR-T cell therapy was 32.2 months (95% CI: 16–48.4) versus 10.5 (95% CI: 7.6–13.4) for those who did not (<i>p</i> < 0.001) (Figure 1E).</p><p>When analyzing whether the patients initially belonged to a CAR-T provider center, we identified better mOS2 for patients from CAR-T cell centers than non-CAR-T provider centers, both among early relapses (25 months [95% CI: 20.6–29.3] vs. 14.9 months [95% CI: 12.2–17.5]; <i>p</i> < 0.001) and late ones (80.7 months [95% CI: 60.1–101.4] vs. 57.7 months [95% CI: 42.4–72.9]; <i>p</i> = 0.011) (Supporting Information S1: Figure 2). Characteristics of both groups are present in Supporting Information S1: Table 6. Interestingly, NT was significantly more commonly used in CAR-T provider centers, especially CAR-T cell therapy.</p><p>Factors related to OS2 are described in Table 1. The multivariable analysis identified early relapse (HR 1.68 [95% CI: 1.37–2.06]; <i>p</i> < 0.001), age over 65 years (HR 1.91 [95% CI: 1.23–2.98]; <i>p</i> = 0.004), treatment with CAR-T cell therapy (HR 0.68 [95% CI: 0.51–0.90]; <i>p</i> = 0.007), and to belong to a CAR-T cell center (HR 0.7 [95% CI: 0.58–0.85]; <i>p</i> < 0.001) as the variables independently related with OS2.</p><p>The advent of NTs in recent years is improving the prognosis of R/R ABCL patients.<span><sup>13, 14</sup></span> Here, we evaluated how these NTs have been used and how much this has impacted patient survival.</p><p>Regarding the time until the first relapse, early relapses during the first year after induction therapy were significantly more frequent, as described previously,<span><sup>15, 16</sup></span> representing 67% of relapses. Likewise, adverse histologies such as HGBCL and T-cell-rich B-cell lymphoma showed a higher frequency of early relapses than DLBCL NOS. Although the greater aggressiveness of these histologies is well known,<span><sup>17, 18</sup></span> these data have not been previously reported to the best of our knowledge. Moreover, we were also able to find a remarkable difference in terms of survival of suffering early versus late relapses, with mOS2 of 13 versus 31 months, respectively. This fact is well known, as previously described in the CORAL and the ORCHARRD trials,<span><sup>15, 16</sup></span> but here, with a median follow-up of more than 4 years, we have demonstrated it in a real-life registry population.</p><p>Regarding age, the proportion between early and late relapses is maintained through the different age ranges but relapses in patients older than 75 years are less frequent. Despite this, as previously described,<span><sup>19</sup></span> patients older than 75 have worse OS than younger ones, among other reasons because they receive in most cases adjusted treatments of less intensity.<span><sup>20</sup></span></p><p>In our series, globally, 32% of the patients received NT. The use of NT has been infrequent in the first relapse. However, it must be considered that only polatuzumab and tafasitamab would be available for this indication. The impact of the use of NT, more widespread from the third line, is reflected in the improvement in the OS2 of these patients compared to those who only receive two lines, as shown in Figure 1A.</p><p>We obtained exciting results regarding how introducing NT has globally improved survival for patients with ABCL. Considering the results of the pivotal trials of NT on this population<span><sup>8-12</sup></span> and the real-world data,<span><sup>21-23</sup></span> it was expected. In this sense, we found that BiMA and CAR-T were related to better outcomes. However, only CAR-T was maintained as an independent variable in the multivariate analysis for those patients who relapsed, although it is important to consider that this therapeutic group was the most represented.</p><p>Finally, we found that patients treated in CAR-T cell centers showed superior survival compared with those treated in non-CAR-T cell centers, which was maintained as an independent variable in the multivariate analysis. These results could be related to several factors. It could represent the advantage of easier or faster access to CAR-T cell therapy but also could be related to the quickest access to new drugs in clinical trials, more common in centers of high complexity. However, with the available data, we cannot rule out that patients treated in CAR centers represent a more selected group with better biology that could explain the improved OS in this group.</p><p>We acknowledge certain limitations in our study. Being a registry study, we do not have detailed data on patient's characteristics or biological features. The total relapse rate is lower than expected, which has to do with patients being diagnosed, especially in large centers, who are finally treated in other centers. On the other hand, we do not have details of the characteristics of the relapse or the complete treatments received. However, this simple analysis has allowed us to analyze a considerable number of patients in a real-world population, and despite the limitations, we have managed to extract precious information.</p><p>In conclusion, our analysis confirms, in a real-world setting, the negative impact of age and timing of relapse on the survival of patients with ABCL. In this regard, histologies such as HGBCL presented more frequent early relapses. Moreover, according to our results, the introduction in recent years of NT has markedly improved survival, especially CAR-T cell therapy.</p><p>Mariana Bastos-Oreiro designed research, performed research, contributed vital new reagents or analytical tools, analyzed data, and wrote the paper. Pau Abrisqueta, Ana Jiménez Ubieto, Maria Poza, María José LLacer, Sonia Gonzalez de Villambrosia, Raúl Córdoba, Alberto López, Elena Ceballos, Belen Navarro, Ana Muntañola, Eva Donato, Eva Diez-Baeza, Lourdes Escoda, Hugo Luzardo, María José Peñarrubia, Daniel García Belmonte, Emilia Pardal, and Claudia Lozada collected data and performed research. Antonio Gutierrez collected data, performed research, and did the statistical analysis. Alejandro Martín García-Sancho designed research analyzed and interpreted data, and wrote the paper.</p><p>The authors declare no conflict of interest.</p><p>This research received no funding.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 4","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2024-04-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.70","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.70","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Aggressive B-cell lymphomas (ABCL) represent a heterogeneous group of biologically different diseases with variable clinical outcomes.1, 2 Around one-third of patients are not cured with frontline treatment, and outcomes for this relapse/refractory (R/R) group are extremely poor with conventional treatments.3-5 However, during the last years, several promising new therapies (NTs) have been progressively incorporated into the treatment arsenal, such as new monoclonal antibodies (MAs), cellular therapy with T cells with chimeric antigen receptor (CAR-T cells), or, in a lesser extent, bispecific antibodies (BiMAs). Polatuzumab vedotin–bendamustine–rituximab6 was approved in Europe since 2019 and funded in Spain since September 2019. Tafasitamab–lenalidomide7 was approved for European Medicines Agency (EMA) in August 2021 and funded in Spain in 2023. CAR-T cell was approved for EMA in 2018,8-10 and funded in Spain in 2019. BiMAs are still only available in clinical trials.11, 12
Our study aims to assess to what extent these new treatments have been incorporated into the clinical practice and how this has impacted patient survival.
This is a multicentre retrospective study based on the GELTAMO RELINF platform, which has been active since January 2014 and includes only essential variables such as histological subtype, age, gender, and current situation. From 60 centers actively registering on the platform invited to participate, 17 centers accepted. All of these centers are university hospitals, and five are CAR-T cell therapy providers. Participating centers completed a short questionnaire on disease relapse and the use of NTs in their registered patients. Conventional treatments only include chemotherapy ± anti-CD20 antibodies ± autologous transplant. Investigators in each center were required to report relapses with histological confirmation of large B-cell lymphoma (LBCL). For refractory patients, histological confirmation was not mandatory. The histologies included were diffuse LBCL (DLBCL) and high-grade B-cell lymphoma (HGBCL) not otherwise specified (NOS) and double hit. Early relapse was defined as within 12 months of completion of induction therapy, and late relapse was defined as more than 12 months.
The present analysis was based on a January 2023 data cut-off. Overall survival (OS) and progression-free survival (PFS) were determined from diagnosis. OS was also calculated since the date of the first relapse (OS2). All reported p values were two-sided, and statistical significance was set at p < 0.05. Analyses were performed using SPSS version 29 (SPSS).
From 3270 patients with ABCL registered, 2853 patients were included in the present analysis; exclusion reasons are described in Supporting Information S1: Table 1.
Supporting Information S1: Table 2 shows patients' characteristics. Three hundred fifty-three patients (47.8%) were identified as primary refractory, whereas 139 patients (19%) relapsed between 3 months and 1 year after completion of induction treatment. These 492 patients were analyzed together as the “early relapse group” (67% of R/R patients). Two hundred and forty-six patients had a late relapse (33%). The distribution was 132 (54%) during the second year, 51 (21%) during the third year, 24 (10%) during the fourth, 16 (6%) during the fifth year, and 23 (10%) from the sixth year onward.
Supporting Information S1: Table 3 describes the characteristics and outcomes of patients who relapsed early and late. A third of relapses were in patients older than 80 years. Regarding histologies, early relapses were most common in double/triple hit HGL (34%) and T-cell rich DLBCL (29%) compared to DLBCL or HGL NOS (16%) (p < 0.001).
Of 738 patients with detailed information on the type of salvage treatments, 236 received NT: 144 received CAR-T (90 as the only NT), 68 BiMAs (27 as the only NT), 92 polatuzumab-based (46 as the only TN), 14 tafasitamab–lenalidomide (12 as the only NT), and 61 received multiple NTs. Specific information on the number of treatment lines was available in 730 of the 738 patients. The median number of lines among R/R patients was 2.1-10 The use of NT was much more frequent in patients who received three or more lines of treatment. The immense majority of patients who received only two treatment lines (n = 376) were treated with conventional treatments (90%), and only 38 (10%) received NT. By contrast, among 354 patients who received more than two lines of treatment, 194 (55%) received NT: 130 (67%) received CAR-T cell therapy (80 as the only NT), 75 (21%) polatuzumab (35 as the only NT), nine (2%) tafasitamab–lenalidomide (seven as the only NT), 55 (15%) BiMA (18 as the only NT), 54 (30%) received multiple NTs, whereas 160 (45%) of these patients did not receive any NT. While 175 (74%) patients received just one NT, 50 (21%) received two combined NTs, and 11 (5%) received three. As shown in Supporting Information S1: Table 4, there were no differences in the timing of relapse (early vs. late) between patients treated with conventional treatments versus NT.
With a median follow-up of 49 months (95% confidence interval, CI: 47–51), the median PFS for the entire cohort was 54 months (95% CI: 48–61), and the median OS was 82 months (95% CI: 74–90) (Supporting Information S1: Figure 1A).
Supporting Information S1: Table 5 shows factors identified as related to OS, since diagnosis. In multivariate analysis, early relapse (hazard ratio, HR 2.91 [95% CI: 2.35–3.6]; p < 0.001), number of total lines (HR 1.4 [95% CI: 1.14–1.71]; p = 0.018), age over 65 years (HR 1.83 [95% CI: 1.17–2.86]; p = 0.008), age over 75 years (HR 2.86 [95% CI: 1.84–4.46]; p < 0.001), use of CAR-T cell therapy (HR 0.67 [95% CI: 0.47–0.96]; p = 0.029), and BiMAs (HR 0.5 [95% CI: 0.37–0.68]; p < 0.001) impacted on OS.
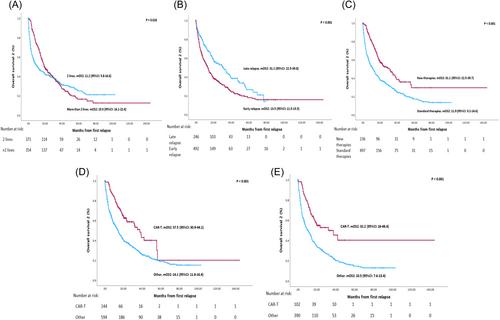
Considering the 738 R/R patients only, with a median follow-up of 40 months, the median OS (mOS2) was 16.8 (95% CI: 14.5–19) months (Supporting Information S1: Figure 1B). It was longer for the group of patients treated with more than two lines (19 months [95% CI: 16–22]) than in patients treated with only two lines (11 months [95% CI: 6–17]; p < 0.001) (Figure 1A).
Median OS2 was significantly shorter (p < 0.001) in the early relapse group (13.5 months [95% CI: 11.5–15.5]) than in late relapses (31.1 months [95% CI: 22.5–39.8]; p < 0.001) (Figure 1B). Median OS2 for relapsed patients treated with NT was 31.1 months (95% CI: 22.5–39.7) compared with 11.9 months (95% CI: 9.2–14.6) for the group of standard treatment (p < 0.001) (Figure 1C). Patients who received CAR-T cell therapy had better OS2 than those who did not (p < 0.001) (Figure 1D). Among early relapses, the median OS2 for patients who received CAR-T cell therapy was 32.2 months (95% CI: 16–48.4) versus 10.5 (95% CI: 7.6–13.4) for those who did not (p < 0.001) (Figure 1E).
When analyzing whether the patients initially belonged to a CAR-T provider center, we identified better mOS2 for patients from CAR-T cell centers than non-CAR-T provider centers, both among early relapses (25 months [95% CI: 20.6–29.3] vs. 14.9 months [95% CI: 12.2–17.5]; p < 0.001) and late ones (80.7 months [95% CI: 60.1–101.4] vs. 57.7 months [95% CI: 42.4–72.9]; p = 0.011) (Supporting Information S1: Figure 2). Characteristics of both groups are present in Supporting Information S1: Table 6. Interestingly, NT was significantly more commonly used in CAR-T provider centers, especially CAR-T cell therapy.
Factors related to OS2 are described in Table 1. The multivariable analysis identified early relapse (HR 1.68 [95% CI: 1.37–2.06]; p < 0.001), age over 65 years (HR 1.91 [95% CI: 1.23–2.98]; p = 0.004), treatment with CAR-T cell therapy (HR 0.68 [95% CI: 0.51–0.90]; p = 0.007), and to belong to a CAR-T cell center (HR 0.7 [95% CI: 0.58–0.85]; p < 0.001) as the variables independently related with OS2.
The advent of NTs in recent years is improving the prognosis of R/R ABCL patients.13, 14 Here, we evaluated how these NTs have been used and how much this has impacted patient survival.
Regarding the time until the first relapse, early relapses during the first year after induction therapy were significantly more frequent, as described previously,15, 16 representing 67% of relapses. Likewise, adverse histologies such as HGBCL and T-cell-rich B-cell lymphoma showed a higher frequency of early relapses than DLBCL NOS. Although the greater aggressiveness of these histologies is well known,17, 18 these data have not been previously reported to the best of our knowledge. Moreover, we were also able to find a remarkable difference in terms of survival of suffering early versus late relapses, with mOS2 of 13 versus 31 months, respectively. This fact is well known, as previously described in the CORAL and the ORCHARRD trials,15, 16 but here, with a median follow-up of more than 4 years, we have demonstrated it in a real-life registry population.
Regarding age, the proportion between early and late relapses is maintained through the different age ranges but relapses in patients older than 75 years are less frequent. Despite this, as previously described,19 patients older than 75 have worse OS than younger ones, among other reasons because they receive in most cases adjusted treatments of less intensity.20
In our series, globally, 32% of the patients received NT. The use of NT has been infrequent in the first relapse. However, it must be considered that only polatuzumab and tafasitamab would be available for this indication. The impact of the use of NT, more widespread from the third line, is reflected in the improvement in the OS2 of these patients compared to those who only receive two lines, as shown in Figure 1A.
We obtained exciting results regarding how introducing NT has globally improved survival for patients with ABCL. Considering the results of the pivotal trials of NT on this population8-12 and the real-world data,21-23 it was expected. In this sense, we found that BiMA and CAR-T were related to better outcomes. However, only CAR-T was maintained as an independent variable in the multivariate analysis for those patients who relapsed, although it is important to consider that this therapeutic group was the most represented.
Finally, we found that patients treated in CAR-T cell centers showed superior survival compared with those treated in non-CAR-T cell centers, which was maintained as an independent variable in the multivariate analysis. These results could be related to several factors. It could represent the advantage of easier or faster access to CAR-T cell therapy but also could be related to the quickest access to new drugs in clinical trials, more common in centers of high complexity. However, with the available data, we cannot rule out that patients treated in CAR centers represent a more selected group with better biology that could explain the improved OS in this group.
We acknowledge certain limitations in our study. Being a registry study, we do not have detailed data on patient's characteristics or biological features. The total relapse rate is lower than expected, which has to do with patients being diagnosed, especially in large centers, who are finally treated in other centers. On the other hand, we do not have details of the characteristics of the relapse or the complete treatments received. However, this simple analysis has allowed us to analyze a considerable number of patients in a real-world population, and despite the limitations, we have managed to extract precious information.
In conclusion, our analysis confirms, in a real-world setting, the negative impact of age and timing of relapse on the survival of patients with ABCL. In this regard, histologies such as HGBCL presented more frequent early relapses. Moreover, according to our results, the introduction in recent years of NT has markedly improved survival, especially CAR-T cell therapy.
Mariana Bastos-Oreiro designed research, performed research, contributed vital new reagents or analytical tools, analyzed data, and wrote the paper. Pau Abrisqueta, Ana Jiménez Ubieto, Maria Poza, María José LLacer, Sonia Gonzalez de Villambrosia, Raúl Córdoba, Alberto López, Elena Ceballos, Belen Navarro, Ana Muntañola, Eva Donato, Eva Diez-Baeza, Lourdes Escoda, Hugo Luzardo, María José Peñarrubia, Daniel García Belmonte, Emilia Pardal, and Claudia Lozada collected data and performed research. Antonio Gutierrez collected data, performed research, and did the statistical analysis. Alejandro Martín García-Sancho designed research analyzed and interpreted data, and wrote the paper.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
