{"title":"Blaschkolinear comedonal nodules and plaques with congenital onset","authors":"Kaan Yilmaz, Leonie Rabe, Cyrill Géraud, Marthe-Lisa Schaarschmidt","doi":"10.1002/jvc2.420","DOIUrl":null,"url":null,"abstract":"<p>A 27-year-old Caucasian male presented with disseminated linear patches of comedones in the head and neck region, on the trunk and extremities. They were readily apparent at birth and have gradually progressed in size whilst being extended by indolent, large nodulocystic lesions during adolescence (Figure 1). He had an unremarkable family history of skin disease and did not report any preexisting conditions. Notably, the patient underwent an excision of a mandibular tumour at the age of 14, which was histologically difficult to classify, but ultimately found to be suggestive of a giant cell granuloma in association with a follicular cyst. No systemic abnormalities, including any visual, skeletal or neurologic impairment, were reported.</p><p>On physical examination, extensive curvilinear, bilateral, mostly alopecic patches of densely distributed open comedones were observed in a Blaschkoid pattern on the face, scalp, neck, trunk and proximal portions of the upper extremities. The scalp and the back were further studded with multiple noninflammatory, partially coalescent cystic nodules reaching up to 6 cm in diameter (Figures 1 and 2). Two skin biopsies were taken from the cystic areas on the back and the occipital region, respectively (Figure 3).</p><p>Naevus comedonicus (NC).</p><p>The histopathologic assessment of the biopsy specimens revealed epidermoid cysts comprising regular stratified squamous epithelium with stratum granulosum and lamellar orthokeratosis (Figure 3). Next-generation sequencing of another skin biopsy specimen from the back yielded the in-frame deletion variant c.1755_1757del p.(Thr586del) in the <i>Never in Mitosis Gene A-Related Kinase 9</i> (<i>NEK9</i>) gene with a mosaic frequency of 30%. In contrast, no pathogenic <i>NEK9</i> variants were identified in DNA extracted from EDTA blood of the patient, indicating a somatic variant in the <i>NEK9</i> gene, which is the molecular aetiology of NC.</p><p>Subsequently, the patient was thoroughly examined for extracutaneous manifestations. In this regard, ophthalmologic evaluation revealed, apart from myopia and astigmatism, no other abnormalities, particularly no cataracts. The echocardiographic assessment showed an annuloaortic ectasia as well as a trivial mitral and tricuspid valve regurgitation, albeit without relevant congenital cardiovascular malformations. Cranial magnetic resonance imaging and computed tomography scan detected no structural changes. No neurologic and skeletal anomalies were found.</p><p>NC (MIM #617025) is a rare organoid epidermal naevus characterized by a hereditary malformation of the pilosebaceous unit, leading to an abrogated production of terminal hair and sebaceous glands.<span><sup>1, 2</sup></span> The histopathologic correlate is the plugging of dilated follicular ostia by lamellar keratinaceous material, which clinically manifests as comedones in a honeycomb pattern, mostly commencing in infancy.<span><sup>3</sup></span> While NC predominantly occurs in a unilateral distribution, bilateral involvement, as in our patient, was reported to account for approximately 35% of the cases.<span><sup>4</sup></span> Three clinical phenotypes of NC have recently been described, that is, (i) predominantly comedonal type, (ii) “Selhorst type” with giant comedones, cysts and nodules with inflammation and scar formation and (iii) atrophoderma vermiculatum-like punctate atrophic scars with comedones.<span><sup>4</sup></span> Although our patient evidently developed a nodulocystic phenotype, no inflammatory activity such as discharge or scarring was observed. In this context, the question arises as to whether the proposed subtypes represent distinct morphological variants or are rather part of a disease continuum with fluctuations and phenotypic shifts, which is deferred to future research. On the other hand, it is important to distinguish between NC and other forms of organoid and nonorganoid (keratinocytic) epidermal nevi, which might similarly present with an extensive Blaschkolinear pattern and/or coexist as a twin spot phenomenon (didymosis).<span><sup>5, 6</sup></span></p><p>The combination of NC and extracutaneous abnormalities is also referred to as naevus comedonicus syndrome (NCS).<span><sup>7</sup></span> Despite the lack of well-defined consensus diagnostic criteria, it has been predominantly associated with ocular, skeletal and neurologic anomalies, whereas ipsilateral cataract is considered the most specific feature of NCS.<span><sup>4, 6, 7</sup></span> In our patient, no sufficient evidence for syndromic involvement was found, although it remains elusive if the mandibular cystic tumour might represent a so far unreported manifestation.</p><p>The Blaschkoid distribution can be attributed to the pathogenic postzygotic mosaicism in the <i>NEK9</i> gene, which was identified as the causative mutation in NC and NCS.<span><sup>8</sup></span> To date, less than 10 <i>NEK9</i> variants have been reported, all of which were restricted to its regulator of chromosome condensation-like (RCC1) and kinase domains.<span><sup>8-10</sup></span> Interestingly, the in-frame deletion p.(Thr586del) in the RCC1 domain of <i>NEK9</i>, which was disclosed in our patient, was hitherto observed in only two other patients with NC and/or NCS.<span><sup>8-10</sup></span> NEK9 belongs to a family of serine-threonine kinases which play a crucial role in checkpoint control and cell cycle regulation.<span><sup>11</sup></span> However, recent evidence suggests that NEK9 might also contribute to follicular homoeostasis, as the gain-of-function mutations in the <i>NEK9</i> gene have been associated with disruption of follicular differentiation in NC.<span><sup>8</sup></span></p><p>Taken together, we herein present a rare case of genetically confirmed NC and lend further evidence for <i>NEK9</i> variants as the molecular basis underlying NC.</p><p>All authors provided care for the patient. Kaan Yilmaz gathered the data and drafted the manuscript. Leonie Rabe, Cyrill Géraud and Marthe-Lisa Schaarschmidt critically revised the manuscript. All authors approved the final version for publication.</p><p>The authors declare no conflict of interest.</p><p>The patient in this manuscript has given written informed consent for participation in the study and the use of his deidentified, anonymized, aggregated data and his case details (including photographs) for publication. Ethical Approval: not applicable.</p>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 4","pages":"1338-1341"},"PeriodicalIF":0.5000,"publicationDate":"2024-04-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.420","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.420","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
A 27-year-old Caucasian male presented with disseminated linear patches of comedones in the head and neck region, on the trunk and extremities. They were readily apparent at birth and have gradually progressed in size whilst being extended by indolent, large nodulocystic lesions during adolescence (Figure 1). He had an unremarkable family history of skin disease and did not report any preexisting conditions. Notably, the patient underwent an excision of a mandibular tumour at the age of 14, which was histologically difficult to classify, but ultimately found to be suggestive of a giant cell granuloma in association with a follicular cyst. No systemic abnormalities, including any visual, skeletal or neurologic impairment, were reported.
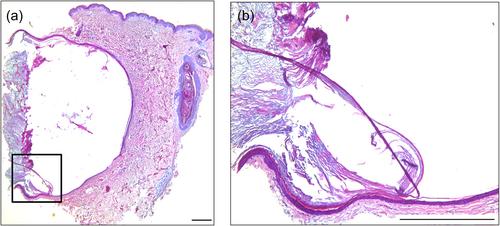
On physical examination, extensive curvilinear, bilateral, mostly alopecic patches of densely distributed open comedones were observed in a Blaschkoid pattern on the face, scalp, neck, trunk and proximal portions of the upper extremities. The scalp and the back were further studded with multiple noninflammatory, partially coalescent cystic nodules reaching up to 6 cm in diameter (Figures 1 and 2). Two skin biopsies were taken from the cystic areas on the back and the occipital region, respectively (Figure 3).
Naevus comedonicus (NC).
The histopathologic assessment of the biopsy specimens revealed epidermoid cysts comprising regular stratified squamous epithelium with stratum granulosum and lamellar orthokeratosis (Figure 3). Next-generation sequencing of another skin biopsy specimen from the back yielded the in-frame deletion variant c.1755_1757del p.(Thr586del) in the Never in Mitosis Gene A-Related Kinase 9 (NEK9) gene with a mosaic frequency of 30%. In contrast, no pathogenic NEK9 variants were identified in DNA extracted from EDTA blood of the patient, indicating a somatic variant in the NEK9 gene, which is the molecular aetiology of NC.
Subsequently, the patient was thoroughly examined for extracutaneous manifestations. In this regard, ophthalmologic evaluation revealed, apart from myopia and astigmatism, no other abnormalities, particularly no cataracts. The echocardiographic assessment showed an annuloaortic ectasia as well as a trivial mitral and tricuspid valve regurgitation, albeit without relevant congenital cardiovascular malformations. Cranial magnetic resonance imaging and computed tomography scan detected no structural changes. No neurologic and skeletal anomalies were found.
NC (MIM #617025) is a rare organoid epidermal naevus characterized by a hereditary malformation of the pilosebaceous unit, leading to an abrogated production of terminal hair and sebaceous glands.1, 2 The histopathologic correlate is the plugging of dilated follicular ostia by lamellar keratinaceous material, which clinically manifests as comedones in a honeycomb pattern, mostly commencing in infancy.3 While NC predominantly occurs in a unilateral distribution, bilateral involvement, as in our patient, was reported to account for approximately 35% of the cases.4 Three clinical phenotypes of NC have recently been described, that is, (i) predominantly comedonal type, (ii) “Selhorst type” with giant comedones, cysts and nodules with inflammation and scar formation and (iii) atrophoderma vermiculatum-like punctate atrophic scars with comedones.4 Although our patient evidently developed a nodulocystic phenotype, no inflammatory activity such as discharge or scarring was observed. In this context, the question arises as to whether the proposed subtypes represent distinct morphological variants or are rather part of a disease continuum with fluctuations and phenotypic shifts, which is deferred to future research. On the other hand, it is important to distinguish between NC and other forms of organoid and nonorganoid (keratinocytic) epidermal nevi, which might similarly present with an extensive Blaschkolinear pattern and/or coexist as a twin spot phenomenon (didymosis).5, 6
The combination of NC and extracutaneous abnormalities is also referred to as naevus comedonicus syndrome (NCS).7 Despite the lack of well-defined consensus diagnostic criteria, it has been predominantly associated with ocular, skeletal and neurologic anomalies, whereas ipsilateral cataract is considered the most specific feature of NCS.4, 6, 7 In our patient, no sufficient evidence for syndromic involvement was found, although it remains elusive if the mandibular cystic tumour might represent a so far unreported manifestation.
The Blaschkoid distribution can be attributed to the pathogenic postzygotic mosaicism in the NEK9 gene, which was identified as the causative mutation in NC and NCS.8 To date, less than 10 NEK9 variants have been reported, all of which were restricted to its regulator of chromosome condensation-like (RCC1) and kinase domains.8-10 Interestingly, the in-frame deletion p.(Thr586del) in the RCC1 domain of NEK9, which was disclosed in our patient, was hitherto observed in only two other patients with NC and/or NCS.8-10 NEK9 belongs to a family of serine-threonine kinases which play a crucial role in checkpoint control and cell cycle regulation.11 However, recent evidence suggests that NEK9 might also contribute to follicular homoeostasis, as the gain-of-function mutations in the NEK9 gene have been associated with disruption of follicular differentiation in NC.8
Taken together, we herein present a rare case of genetically confirmed NC and lend further evidence for NEK9 variants as the molecular basis underlying NC.
All authors provided care for the patient. Kaan Yilmaz gathered the data and drafted the manuscript. Leonie Rabe, Cyrill Géraud and Marthe-Lisa Schaarschmidt critically revised the manuscript. All authors approved the final version for publication.
The authors declare no conflict of interest.
The patient in this manuscript has given written informed consent for participation in the study and the use of his deidentified, anonymized, aggregated data and his case details (including photographs) for publication. Ethical Approval: not applicable.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
