{"title":"Risk model for morbidity and mortality following liver surgery based on a national Japanese database","authors":"Tatsuya Orimo, Shinya Hirakawa, Akinobu Taketomi, Hisateru Tachimori, Taro Oshikiri, Hiroaki Miyata, Yoshihiro Kakeji, Ken Shirabe","doi":"10.1002/ags3.12803","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>We evaluated the morbidity and mortality associated with liver surgery in Japan and developed a risk model for liver resection using information from a national database.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We retrospectively reviewed 73 861 Japanese patients who underwent hepatectomy between 2014 and 2019, using information from the National Clinical Database (NCD) registrations. The primary endpoints were 30 days and in-hospital mortality, and the secondary endpoints were postoperative complications. Logistic regression risk models for postoperative morbidity and mortality after hepatectomy were constructed based on preoperative clinical parameters and types of liver resection, and validated using a bootstrapping method.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The 30-day and in-hospital mortality rates were 0.9% and 1.7%, respectively. Trisectionectomy, hepatectomy for gallbladder cancer, hepatectomy for perihilar cholangiocarcinoma, and poor activities of daily living were statistically significant risk factors with high odds ratios for both postoperative morbidity and mortality. Internal validations indicated that the c-indices for 30-day and in-hospital mortality were 0.824 and 0.839, respectively.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>We developed a risk model for liver resection by using a national surgical database that can predict morbidity and mortality based on preoperative factors.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 5","pages":"896-916"},"PeriodicalIF":3.3000,"publicationDate":"2024-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12803","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12803","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Aim
We evaluated the morbidity and mortality associated with liver surgery in Japan and developed a risk model for liver resection using information from a national database.
Methods
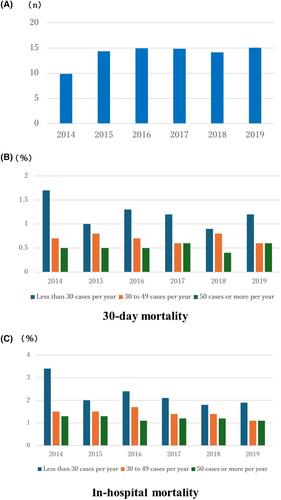
We retrospectively reviewed 73 861 Japanese patients who underwent hepatectomy between 2014 and 2019, using information from the National Clinical Database (NCD) registrations. The primary endpoints were 30 days and in-hospital mortality, and the secondary endpoints were postoperative complications. Logistic regression risk models for postoperative morbidity and mortality after hepatectomy were constructed based on preoperative clinical parameters and types of liver resection, and validated using a bootstrapping method.
Results
The 30-day and in-hospital mortality rates were 0.9% and 1.7%, respectively. Trisectionectomy, hepatectomy for gallbladder cancer, hepatectomy for perihilar cholangiocarcinoma, and poor activities of daily living were statistically significant risk factors with high odds ratios for both postoperative morbidity and mortality. Internal validations indicated that the c-indices for 30-day and in-hospital mortality were 0.824 and 0.839, respectively.
Conclusions
We developed a risk model for liver resection by using a national surgical database that can predict morbidity and mortality based on preoperative factors.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
