{"title":"Richter transformation acquiring PLCG2 mutation during Bruton tyrosine kinase inhibitors treatment","authors":"Takafumi Tsushima, Nobue Sato, Yong-Mei Guo, Hirotaka Nakamura, Kodai Kunisada, Song-Gi Chi, Kenta Akie, Yuki Takahashi, Saki Nakamura, Kaoru Shimada, Genichiro Ishii, Yosuke Minami, Junichiro Yuda","doi":"10.1002/jha2.891","DOIUrl":null,"url":null,"abstract":"<p>The incidence of Richter transformation in relapsed/refractory chronic lymphocytic leukemia (CLL) is up to 15% and Richter transformation is a frequent cause of treatment failure on ibrutinib (IBR) [<span>1</span>]. IBR has been promising in CLL cell growth suppression by inhibiting Bruton tyrosine kinase (<i>BTK</i>) [<span>2</span>]. However, resistance can occur due to specific mutations in <i>BTK</i> or <i>PLCG2</i> genes [<span>3</span>]. Another agent, venetoclax (VEN) has shown excellent efficacy in relapsed refractory CLL [<span>4</span>]. In Richter transformation, the effectiveness of VEN alone or in combination with conventional chemotherapy has been demonstrated, although research in this area is limited and based on only a few cases [<span>5-7</span>]. <i>BTK</i>/<i>PLCG2</i> mutations play a role in IBR-resistant CLL progression. However, there is limited knowledge about <i>BTK</i> or <i>PLCG2</i> gene mutation statuses in Richter transformation.</p><p>A 72-year-old male was diagnosed with CLL characterized by a deletion in chromosome 17p [del(17p)] and a complex karyotype. After 12 months of diagnosis, he started IBR treatment. He initially showed a partial response. Two years after starting IBR, CLL cells in the peripheral blood increased, and he developed bilateral cervical lymphadenopathy, along with elevated levels of lactate dehydrogenase (LDH) and soluble interleukin-2 receptor (sIL-2R). Fluorodeoxyglucose-positron emission tomography (FDG-PET) revealed systemic lymphadenopathy. Bone marrow examination showed increased atypical lymphocytes, displaying a CD5+CD10-19+sIgκ+ phenotype, with del(17p) present in 27% of all nucleated cells, as confirmed by fluorescence in situ hybridization. The pathological examination of the cervical lymph nodes showed a diffuse proliferation of large lymphocytes that tested positive for CD5, CD19, CD20, CD22, CD23, CD45, and BCL-2 and negative for MUM-1 and BCL-6, with a Ki-67 index of ∼50%. A biopsy confirmed the transformation into diffuse large B-cell lymphoma (Figure 1). Genetic testing was conducted on lymph nodes and bone marrow samples collected simultaneously; <i>TP53</i> mutation (R283P) was found in lymph nodes [variant allele frequency (VAF): 0.85] and bone marrow specimens (VAF: 0.77). However, <i>PLCG2</i> mutation (D1144G) was only detected in the lymph node specimens (VAF: 0.07). In this case, a targeted gene panel was used in Japan. The sensitivity of allele mutation detection was 0.05. A single polymerase chain reaction was not performed. Additionally, we could not measure the <i>IGHV</i> mutation.</p><p>The patient's treatment involved VEN usage for gradually increasing doses up to 200 mg (with fluconazole concomitant use) as per guidelines, while the use of IBR gradually reduced (Figure 2). The patient's clinical symptoms (fever and others) and lymphadenopathy showed no signs of improvement with VEN initiation and IBR dose reduction. The laboratory values indicated a worsening trend, with elevated LDH and sIL-2R, reaching 511 U/L (normal; 124–222 IU/L) and 4,247 U/mL (normal; 122–496 U/mL), respectively. Initially, the plan was to taper off IBR, but due to worsening CLL lesions (especially the presence of leukemic cells in the peripheral blood and bone marrow), IBR was continued at 420 mg/day in combination with 200 mg/day VEN. Subsequently, there was a marked improvement in the peripheral blood and lymph node lesions. This suggests that VEN is highly effective against Richter transformation, while IBR remains effective in treating existing CLL lesions in the bone marrow since no <i>PLCG2</i> mutations were found. Following VEN initiation, RIT was administered every 4 weeks for six doses, initiated 6 months after VEN treatment began. At the end of RIT, FDG-PET and bone marrow examination confirmed that the patient achieved complete remission, which was maintained at 24 months post-treatment follow-up. During the treatment course, neutropenia of CTCAE Grade1 was observed, and events such as febrile neutropenia and infection were not observed. Blood count has recovered to normal range at CR. At that time, peripheral blood flow cytometry-minimal residual disease (MRD) was negative.</p><p>This case represents a rare report of a <i>PLCG2</i> mutation specifically appearing only in the lymph nodes and not in the bone marrow during IBR treatment for CLL, leading to Richter transformation. The patient had complex karyotype and <i>TP53</i> abnormalities during the initial treatment, indicating a potential for a shorter duration of response compared to typical cases [<span>8</span>]. Despite approximately 2 years of disease control with IBR, the patient eventually progressed to Richter transformation, with an IBR-resistant <i>PLCG2</i> mutation detected in the lymph node lesions. CLL is known to exhibit genomic instability and clonal evolution, which can lead to the development of Richter transformation [<span>9</span>]. Richter transformation from CLL is associated with <i>TP53</i>, <i>NOTCH1</i> mutation, <i>CDKN2A</i> deletion, and <i>MYC</i> translocation [<span>10</span>]. Conventional cytotoxic anticancer treatments for Richter transformation have demonstrated unsatisfactory results, highlighting the need for new and innovative therapies [<span>11</span>]. In our patient, <i>PLCG2</i> mutations were detected only in the lymph node lesions, where more aggressive Richter transformation findings were observed, while no mutation was found in the bone marrow specimens; this aligns with the clinical course, which showed a transient increase in CLL cells in the peripheral blood after discontinuing IBR treatment. The three-drug combination therapy of IBR + VEN + RIT has effectively maintained a long-term complete remission in this patient. This case represents the first report of a patient with Richter transformation with differing <i>PLCG2</i> mutation statuses between the bone marrow and lymph nodes.</p><p>The combination of VEN and IBR has been documented to effectively reduce the resting and dividing subpopulations in most cases, making it a significant treatment approach for CLL [<span>12</span>]. In a particular study, high MRD-negative rates were achieved with the two-drug combination of IBR and VEN [<span>13</span>]. There are also reports of triple therapy with obinutuzumab, IBR, and VEN, which achieved negative MRD with high safety in high-risk CLL patients, suggesting earlier initiation of multidrug combination therapy is also promising [<span>14</span>]. In conclusion, this report highlights the effectiveness of VEN and RIT even in cases of Richter transformation with <i>PLCG2</i> mutations that have developed resistance to IBR. Furthermore, the results indicate that IBR remains significantly effective in treating existing residual CLL lesions in Richter transformation.</p><p>Takafumi Tsushima collected the data and wrote the manuscript. Junichiro Yuda and Takafumi Tsushima provided patient care. All the authors have reviewed and approved the final manuscript.</p><p>The authors declare no conflict of interest.</p><p>All procedures were performed according to the ethical standards of the institutional and national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the institutional review board.</p><p>The author has confirmed patient consent statement is not needed for this submission.</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>","PeriodicalId":72883,"journal":{"name":"EJHaem","volume":"5 3","pages":"642-645"},"PeriodicalIF":1.2000,"publicationDate":"2024-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.891","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EJHaem","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jha2.891","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
The incidence of Richter transformation in relapsed/refractory chronic lymphocytic leukemia (CLL) is up to 15% and Richter transformation is a frequent cause of treatment failure on ibrutinib (IBR) [1]. IBR has been promising in CLL cell growth suppression by inhibiting Bruton tyrosine kinase (BTK) [2]. However, resistance can occur due to specific mutations in BTK or PLCG2 genes [3]. Another agent, venetoclax (VEN) has shown excellent efficacy in relapsed refractory CLL [4]. In Richter transformation, the effectiveness of VEN alone or in combination with conventional chemotherapy has been demonstrated, although research in this area is limited and based on only a few cases [5-7]. BTK/PLCG2 mutations play a role in IBR-resistant CLL progression. However, there is limited knowledge about BTK or PLCG2 gene mutation statuses in Richter transformation.
A 72-year-old male was diagnosed with CLL characterized by a deletion in chromosome 17p [del(17p)] and a complex karyotype. After 12 months of diagnosis, he started IBR treatment. He initially showed a partial response. Two years after starting IBR, CLL cells in the peripheral blood increased, and he developed bilateral cervical lymphadenopathy, along with elevated levels of lactate dehydrogenase (LDH) and soluble interleukin-2 receptor (sIL-2R). Fluorodeoxyglucose-positron emission tomography (FDG-PET) revealed systemic lymphadenopathy. Bone marrow examination showed increased atypical lymphocytes, displaying a CD5+CD10-19+sIgκ+ phenotype, with del(17p) present in 27% of all nucleated cells, as confirmed by fluorescence in situ hybridization. The pathological examination of the cervical lymph nodes showed a diffuse proliferation of large lymphocytes that tested positive for CD5, CD19, CD20, CD22, CD23, CD45, and BCL-2 and negative for MUM-1 and BCL-6, with a Ki-67 index of ∼50%. A biopsy confirmed the transformation into diffuse large B-cell lymphoma (Figure 1). Genetic testing was conducted on lymph nodes and bone marrow samples collected simultaneously; TP53 mutation (R283P) was found in lymph nodes [variant allele frequency (VAF): 0.85] and bone marrow specimens (VAF: 0.77). However, PLCG2 mutation (D1144G) was only detected in the lymph node specimens (VAF: 0.07). In this case, a targeted gene panel was used in Japan. The sensitivity of allele mutation detection was 0.05. A single polymerase chain reaction was not performed. Additionally, we could not measure the IGHV mutation.
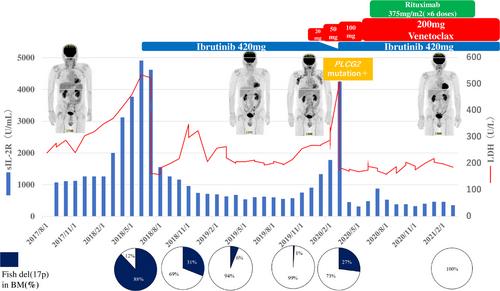
The patient's treatment involved VEN usage for gradually increasing doses up to 200 mg (with fluconazole concomitant use) as per guidelines, while the use of IBR gradually reduced (Figure 2). The patient's clinical symptoms (fever and others) and lymphadenopathy showed no signs of improvement with VEN initiation and IBR dose reduction. The laboratory values indicated a worsening trend, with elevated LDH and sIL-2R, reaching 511 U/L (normal; 124–222 IU/L) and 4,247 U/mL (normal; 122–496 U/mL), respectively. Initially, the plan was to taper off IBR, but due to worsening CLL lesions (especially the presence of leukemic cells in the peripheral blood and bone marrow), IBR was continued at 420 mg/day in combination with 200 mg/day VEN. Subsequently, there was a marked improvement in the peripheral blood and lymph node lesions. This suggests that VEN is highly effective against Richter transformation, while IBR remains effective in treating existing CLL lesions in the bone marrow since no PLCG2 mutations were found. Following VEN initiation, RIT was administered every 4 weeks for six doses, initiated 6 months after VEN treatment began. At the end of RIT, FDG-PET and bone marrow examination confirmed that the patient achieved complete remission, which was maintained at 24 months post-treatment follow-up. During the treatment course, neutropenia of CTCAE Grade1 was observed, and events such as febrile neutropenia and infection were not observed. Blood count has recovered to normal range at CR. At that time, peripheral blood flow cytometry-minimal residual disease (MRD) was negative.
This case represents a rare report of a PLCG2 mutation specifically appearing only in the lymph nodes and not in the bone marrow during IBR treatment for CLL, leading to Richter transformation. The patient had complex karyotype and TP53 abnormalities during the initial treatment, indicating a potential for a shorter duration of response compared to typical cases [8]. Despite approximately 2 years of disease control with IBR, the patient eventually progressed to Richter transformation, with an IBR-resistant PLCG2 mutation detected in the lymph node lesions. CLL is known to exhibit genomic instability and clonal evolution, which can lead to the development of Richter transformation [9]. Richter transformation from CLL is associated with TP53, NOTCH1 mutation, CDKN2A deletion, and MYC translocation [10]. Conventional cytotoxic anticancer treatments for Richter transformation have demonstrated unsatisfactory results, highlighting the need for new and innovative therapies [11]. In our patient, PLCG2 mutations were detected only in the lymph node lesions, where more aggressive Richter transformation findings were observed, while no mutation was found in the bone marrow specimens; this aligns with the clinical course, which showed a transient increase in CLL cells in the peripheral blood after discontinuing IBR treatment. The three-drug combination therapy of IBR + VEN + RIT has effectively maintained a long-term complete remission in this patient. This case represents the first report of a patient with Richter transformation with differing PLCG2 mutation statuses between the bone marrow and lymph nodes.
The combination of VEN and IBR has been documented to effectively reduce the resting and dividing subpopulations in most cases, making it a significant treatment approach for CLL [12]. In a particular study, high MRD-negative rates were achieved with the two-drug combination of IBR and VEN [13]. There are also reports of triple therapy with obinutuzumab, IBR, and VEN, which achieved negative MRD with high safety in high-risk CLL patients, suggesting earlier initiation of multidrug combination therapy is also promising [14]. In conclusion, this report highlights the effectiveness of VEN and RIT even in cases of Richter transformation with PLCG2 mutations that have developed resistance to IBR. Furthermore, the results indicate that IBR remains significantly effective in treating existing residual CLL lesions in Richter transformation.
Takafumi Tsushima collected the data and wrote the manuscript. Junichiro Yuda and Takafumi Tsushima provided patient care. All the authors have reviewed and approved the final manuscript.
The authors declare no conflict of interest.
All procedures were performed according to the ethical standards of the institutional and national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the institutional review board.
The author has confirmed patient consent statement is not needed for this submission.
The authors have confirmed clinical trial registration is not needed for this submission.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
