Mark Ayoub, Carol Faris, Julton Tomanguillo Chumbe, Ebubekir Daglilar, Nadeem Anwar, Vishnu Naravadi
{"title":"Safety of DOACs in patients with Child-Pugh Class C cirrhosis and trial fibrillation","authors":"Mark Ayoub, Carol Faris, Julton Tomanguillo Chumbe, Ebubekir Daglilar, Nadeem Anwar, Vishnu Naravadi","doi":"10.1002/jgh3.13074","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Anticoagulation (AC) is used for stroke prevention in atrial fibrillation (AF). Direct Oral Anticoagulants (DOACs) are safe in patients with AF without cirrhosis, they are hardly studied in patients with advanced cirrhosis. Our study evaluates the safety and outcomes of DOACs in patients with Child-Pugh class C cirrhosis (CPC).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We queried TriNetX Database. Patients with CPC and AF were divided into three cohorts: patients on DOACs, no AC, and warfarin. Three study arms were created using a 1:1 propensity score matching system (PSM).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Totally 16 029 patients met the inclusion criteria. Of those, 20.2% (<i>n</i> = 3235) were on DOACs, 47.1% (<i>n</i> = 7552) were not on AC, and 32.7% (<i>n</i> = 5242) were on warfarin. First arm comparing AC <i>versus</i> no AC, a statistically significant benefit was identified in 3-year mortality risk (47% <i>vs</i> 71%, <i>P</i> < 0.0001) and transplant status (17% <i>vs</i> 5%, p < 0.0001) with AC. However, no significant difference was identified regarding intracranial hemorrhage and GI bleeding risk. Second arm comparing patients on DOACs <i>versus</i> no AC, we identified mortality benefit (40% <i>vs</i> 72%, <i>P</i> < 0.0001) and a higher transplant rate (9% <i>vs</i> 3.2%, <i>P</i> < 0.0001) with DOACs. Intracranial hemorrhage rates (6% <i>vs</i> 4%, <i>P</i> = 0.03) were higher in patients on DOACs. Third arm comparing patients on DOACs <i>versus</i> Warfarin, a statistically significant lower risk of intracranial hemorrhage (6.6% <i>vs</i> 8.7%, <i>P</i> = 0.004) and GI bleed (2% <i>vs</i> 2.4%, <i>P</i> < 0.0001) were identified in patients on DOACs.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Anticoagulation is safe in patients with CPC with AF and may provide a mortality benefit. DOACs are a safer alternative to warfarin.</p>\n </section>\n </div>","PeriodicalId":45861,"journal":{"name":"JGH Open","volume":"8 5","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2024-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgh3.13074","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JGH Open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.13074","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Anticoagulation (AC) is used for stroke prevention in atrial fibrillation (AF). Direct Oral Anticoagulants (DOACs) are safe in patients with AF without cirrhosis, they are hardly studied in patients with advanced cirrhosis. Our study evaluates the safety and outcomes of DOACs in patients with Child-Pugh class C cirrhosis (CPC).
Methods
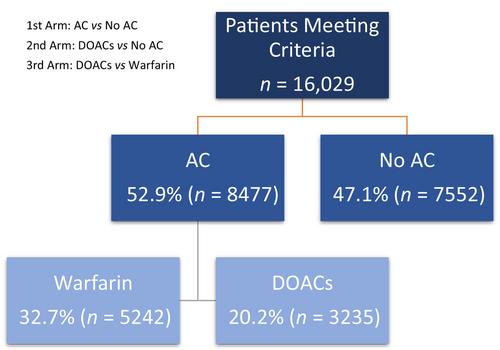
We queried TriNetX Database. Patients with CPC and AF were divided into three cohorts: patients on DOACs, no AC, and warfarin. Three study arms were created using a 1:1 propensity score matching system (PSM).
Results
Totally 16 029 patients met the inclusion criteria. Of those, 20.2% (n = 3235) were on DOACs, 47.1% (n = 7552) were not on AC, and 32.7% (n = 5242) were on warfarin. First arm comparing AC versus no AC, a statistically significant benefit was identified in 3-year mortality risk (47% vs 71%, P < 0.0001) and transplant status (17% vs 5%, p < 0.0001) with AC. However, no significant difference was identified regarding intracranial hemorrhage and GI bleeding risk. Second arm comparing patients on DOACs versus no AC, we identified mortality benefit (40% vs 72%, P < 0.0001) and a higher transplant rate (9% vs 3.2%, P < 0.0001) with DOACs. Intracranial hemorrhage rates (6% vs 4%, P = 0.03) were higher in patients on DOACs. Third arm comparing patients on DOACs versus Warfarin, a statistically significant lower risk of intracranial hemorrhage (6.6% vs 8.7%, P = 0.004) and GI bleed (2% vs 2.4%, P < 0.0001) were identified in patients on DOACs.
Conclusion
Anticoagulation is safe in patients with CPC with AF and may provide a mortality benefit. DOACs are a safer alternative to warfarin.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
