Sustaining HIV service delivery to key population clients using client-centered models during the debate and enactment of the Anti-Homosexuality Act in Uganda
Vamsi Vasireddy, Natalie E. Brown, Neha Shah, Trevor A. Crowell
{"title":"Sustaining HIV service delivery to key population clients using client-centered models during the debate and enactment of the Anti-Homosexuality Act in Uganda","authors":"Vamsi Vasireddy, Natalie E. Brown, Neha Shah, Trevor A. Crowell","doi":"10.1002/jia2.26253","DOIUrl":null,"url":null,"abstract":"<p>Punitive and discriminatory laws against key populations (KP), particularly men who have sex with men (MSM), have been on the rise for over a decade [<span>1, 2</span>]. Studies have shown these laws to be associated with healthcare avoidance, decreased HIV testing and increased HIV prevalence [<span>3-5</span>]. These laws further marginalize groups that are disproportionately affected by HIV [<span>6</span>-7] and imperil the achievement of the UNAIDS 95-95-95 targets [<span>8</span>].</p><p>In Uganda, same-sex relationships have been illegal since the early 20th century. In 2010, a newspaper infamously outed 100 alleged homosexuals, driving many into hiding [<span>9</span>]. The 2014 Anti-Homosexuality Act (AHA), colloquially known as the “Kill the Gays” bill, penalized consensual same-sex sexual acts with death or life imprisonment, but was struck down by the Constitutional Court. Ugandan media started discussing a possible new AHA in December 2022. On 21 March 2023, Parliament overwhelmingly passed a new AHA, which was signed into law on 26 May 2023. The 2023 AHA criminalizes same-sex sexual acts with sentences ranging from 10-year imprisonment to death. It also criminalizes the promotion of homosexuality, which is broad enough to include routine public health activities, such as HIV prevention, safer sex education and community engagement. This creates opportunities for abuse, puts organizations delivering healthcare to MSM in danger of prosecution and impedes access to KP-friendly services. On 3 April 2024, following a lengthy legal challenge, the Ugandan Constitutional Court upheld the majority of the AHA, leaving in place problematic sections of AHA including the prohibition against “promotion of homosexuality,” the use of the death penalty for repeat offenders engaging in consensual sexual contact and allowing for “rehabilitation” of LGBTQI+ persons.</p><p>The United States President's Emergency Plan for AIDS Relief (PEPFAR) supports over 1.3 million Ugandans on antiretroviral therapy (ART). In 2023, PEPFAR supported 84 drop-in-centres (DICs) across Uganda that provided comprehensive HIV prevention and treatment services for KP clients. The DICs were unnamed/unidentified to create confidential and safe spaces for KP clients, including MSM, female sex workers (FSWs) and transgender persons. DICs were strategically situated for easy access and staffed by at least one nurse and a mix of community health workers, including peers within the KP communities. Service delivery data from DICs were de-identified, disaggregated by type of KP clients and services, and uploaded to a central database. Following concerns raised by KP clients regarding healthcare access, we initiated monitoring of AHA impacts on HIV service delivery and implemented new adaptations to support care delivery.</p><p>This report focuses on three DICs operated by a single agency that provided consistent data and served a representative population of KP clients. A larger sample was not possible due to inconsistent data access and the sensitive nature of DIC locations and operations. We noticed a steep decline in DIC visits coinciding with escalating anti-homosexual sentiment and reporting in the media (Figure 1). At least four DICs closed during this time due to safety incidents. Numerous MSM reported evictions from their residences and assault. The PEPFAR programme quickly pivoted its models to support KP clients as described below.</p><p>With these programme adaptations, the DICs analysed here started seeing a return of KP clients that was maintained through the end of observation in November 2023. However, anecdotally, the effect has not been consistent across all DICs and others have not seen the same return of clients. The DICs are located across Uganda with varying community engagement and resistance. Some communities did not want data reported from the DICs due to fear of identification. PEPFAR respected these community preferences. Support from local governments also varied across the country, with some district leadership and police actively opposing DIC operations.</p><p>As KP communities continue to face stigma, discrimination and punitive legislation, it is important that PEPFAR adapt to maintain the delivery of life-saving healthcare services. PEPFAR continues to monitor service delivery and utilization weekly to ensure quick adaptation of services, despite the negative impacts of the AHA. Our experience in Uganda can inform efforts to maintain resilient healthcare systems and services for KP clients in the face of growing punitive and discriminatory legislations in other countries. Countries facing such situations might employ similar monitoring procedures and implement similar programme adaptations to mitigate the impact of harmful legislations. Community engagement and inputs are critical for KP-friendly services that reach the clients through outreach methods if the clients are fearful of accessing a health facility. Programmes and funders must be flexible to quickly adapt service delivery initiatives without red tape. Lastly, high-level advocacy from funders and diplomatic partners should continue for upholding human rights and equitable healthcare access for all.</p><p>The authors have no competing interests to declare.</p><p>VV conceived of this work, conducted the analyses and authored the original draft of the manuscript. NEB provided resources and methodologic input. NS provided administrative support to the project, methodologic input and supervision of the work. TAC provided methodologic input and supervision of the work. All authors assisted in the writing, review, and editing of the manuscript and approved the manuscript for publication in its final form.</p><p>This work was supported by the President's Emergency Plan for AIDS Relief via a cooperative agreement between the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. and the US Department of Defense (W81XWH-18-2-0040).</p><p>The views expressed are those of the authors and should not be construed to represent the positions of the US Army, the Department of Defense, the Department of State or the Henry M. Jackson Foundation for the Advancement of Military Medicine.</p><p>This work was presented, in part, at the 12th IAS Conference on HIV Science in Brisbane, Australia, 23–26 July 2023.</p>","PeriodicalId":201,"journal":{"name":"Journal of the International AIDS Society","volume":"27 5","pages":""},"PeriodicalIF":4.9000,"publicationDate":"2024-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jia2.26253","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the International AIDS Society","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jia2.26253","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Punitive and discriminatory laws against key populations (KP), particularly men who have sex with men (MSM), have been on the rise for over a decade [1, 2]. Studies have shown these laws to be associated with healthcare avoidance, decreased HIV testing and increased HIV prevalence [3-5]. These laws further marginalize groups that are disproportionately affected by HIV [6-7] and imperil the achievement of the UNAIDS 95-95-95 targets [8].
In Uganda, same-sex relationships have been illegal since the early 20th century. In 2010, a newspaper infamously outed 100 alleged homosexuals, driving many into hiding [9]. The 2014 Anti-Homosexuality Act (AHA), colloquially known as the “Kill the Gays” bill, penalized consensual same-sex sexual acts with death or life imprisonment, but was struck down by the Constitutional Court. Ugandan media started discussing a possible new AHA in December 2022. On 21 March 2023, Parliament overwhelmingly passed a new AHA, which was signed into law on 26 May 2023. The 2023 AHA criminalizes same-sex sexual acts with sentences ranging from 10-year imprisonment to death. It also criminalizes the promotion of homosexuality, which is broad enough to include routine public health activities, such as HIV prevention, safer sex education and community engagement. This creates opportunities for abuse, puts organizations delivering healthcare to MSM in danger of prosecution and impedes access to KP-friendly services. On 3 April 2024, following a lengthy legal challenge, the Ugandan Constitutional Court upheld the majority of the AHA, leaving in place problematic sections of AHA including the prohibition against “promotion of homosexuality,” the use of the death penalty for repeat offenders engaging in consensual sexual contact and allowing for “rehabilitation” of LGBTQI+ persons.
The United States President's Emergency Plan for AIDS Relief (PEPFAR) supports over 1.3 million Ugandans on antiretroviral therapy (ART). In 2023, PEPFAR supported 84 drop-in-centres (DICs) across Uganda that provided comprehensive HIV prevention and treatment services for KP clients. The DICs were unnamed/unidentified to create confidential and safe spaces for KP clients, including MSM, female sex workers (FSWs) and transgender persons. DICs were strategically situated for easy access and staffed by at least one nurse and a mix of community health workers, including peers within the KP communities. Service delivery data from DICs were de-identified, disaggregated by type of KP clients and services, and uploaded to a central database. Following concerns raised by KP clients regarding healthcare access, we initiated monitoring of AHA impacts on HIV service delivery and implemented new adaptations to support care delivery.
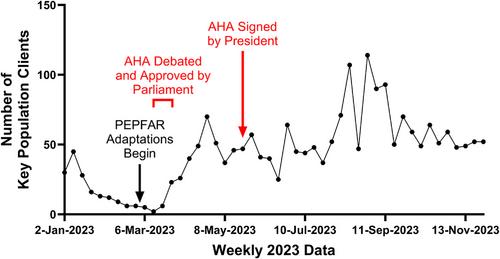
This report focuses on three DICs operated by a single agency that provided consistent data and served a representative population of KP clients. A larger sample was not possible due to inconsistent data access and the sensitive nature of DIC locations and operations. We noticed a steep decline in DIC visits coinciding with escalating anti-homosexual sentiment and reporting in the media (Figure 1). At least four DICs closed during this time due to safety incidents. Numerous MSM reported evictions from their residences and assault. The PEPFAR programme quickly pivoted its models to support KP clients as described below.
With these programme adaptations, the DICs analysed here started seeing a return of KP clients that was maintained through the end of observation in November 2023. However, anecdotally, the effect has not been consistent across all DICs and others have not seen the same return of clients. The DICs are located across Uganda with varying community engagement and resistance. Some communities did not want data reported from the DICs due to fear of identification. PEPFAR respected these community preferences. Support from local governments also varied across the country, with some district leadership and police actively opposing DIC operations.
As KP communities continue to face stigma, discrimination and punitive legislation, it is important that PEPFAR adapt to maintain the delivery of life-saving healthcare services. PEPFAR continues to monitor service delivery and utilization weekly to ensure quick adaptation of services, despite the negative impacts of the AHA. Our experience in Uganda can inform efforts to maintain resilient healthcare systems and services for KP clients in the face of growing punitive and discriminatory legislations in other countries. Countries facing such situations might employ similar monitoring procedures and implement similar programme adaptations to mitigate the impact of harmful legislations. Community engagement and inputs are critical for KP-friendly services that reach the clients through outreach methods if the clients are fearful of accessing a health facility. Programmes and funders must be flexible to quickly adapt service delivery initiatives without red tape. Lastly, high-level advocacy from funders and diplomatic partners should continue for upholding human rights and equitable healthcare access for all.
The authors have no competing interests to declare.
VV conceived of this work, conducted the analyses and authored the original draft of the manuscript. NEB provided resources and methodologic input. NS provided administrative support to the project, methodologic input and supervision of the work. TAC provided methodologic input and supervision of the work. All authors assisted in the writing, review, and editing of the manuscript and approved the manuscript for publication in its final form.
This work was supported by the President's Emergency Plan for AIDS Relief via a cooperative agreement between the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. and the US Department of Defense (W81XWH-18-2-0040).
The views expressed are those of the authors and should not be construed to represent the positions of the US Army, the Department of Defense, the Department of State or the Henry M. Jackson Foundation for the Advancement of Military Medicine.
This work was presented, in part, at the 12th IAS Conference on HIV Science in Brisbane, Australia, 23–26 July 2023.
期刊介绍:
The Journal of the International AIDS Society (JIAS) is a peer-reviewed and Open Access journal for the generation and dissemination of evidence from a wide range of disciplines: basic and biomedical sciences; behavioural sciences; epidemiology; clinical sciences; health economics and health policy; operations research and implementation sciences; and social sciences and humanities. Submission of HIV research carried out in low- and middle-income countries is strongly encouraged.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
