Alfred Lok Hang Lee, Eddie Chi Man Leung, Viola Chi Ying Chow
{"title":"Comparison of carbapenem MIC for NDM-producing Enterobacterales by different AST methods.","authors":"Alfred Lok Hang Lee, Eddie Chi Man Leung, Viola Chi Ying Chow","doi":"10.1093/jacamr/dlae028","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>This study compared the performance of MIC test strip (ETEST), automated AST card (Vitek 2) and broth microdilution (BMD) in determining carbapenem susceptibility and MIC values of NDM-producing Enterobacterales.</p><p><strong>Methods: </strong>NDM-producing Enterobacterales recovered from clinical specimens were included. The presence of <i>bla</i><sub>NDM</sub> was confirmed by PCR. Identification of bacterial isolates was done by MALDI-TOF. Phenotypic susceptibility to three carbapenems (ertapenem, imipenem and meropenem) was tested by BMD, ETEST and Vitek 2. MIC values were interpreted in accordance with CLSI M100 (2022 edition). Using BMD as the reference standard, the essential agreement (EA), categorical agreement (CA), very major error (VME) and major error (ME) rates were evaluated.</p><p><strong>Results: </strong>Forty-seven NDM-producing Enterobacterales isolates were included, 44 of which were <i>Escherichia coli</i>. The EA of Vitek 2 was 97.9% for ertapenem, 25.5% for meropenem and 42.6% for imipenem. Using Vitek 2, there were 0% VMEs across all three carbapenems tested. The EA of ETEST was 53.2% for ertapenem, 55.3% for imipenem and 36.2% for meropenem. The rates of VMEs for ETEST were high too (ertapenem 8.5%, meropenem 36.2%, imipenem 26.1%). The MIC values obtained from Vitek 2 were consistently higher than those from BMD, while MICs from ETEST were consistently lower than those from BMD.</p><p><strong>Conclusions: </strong>The VME rate for ETEST was unacceptably high when BMD was used as the standard for comparison. Vitek 2 had acceptable EA and CA for ertapenem when BMD was used as the standard for comparison. For meropenem and imipenem, neither of the methods (ETEST, Vitek 2) showed acceptable EA and CA when compared with BMD.</p>","PeriodicalId":14594,"journal":{"name":"JAC-Antimicrobial Resistance","volume":"6 2","pages":"dlae028"},"PeriodicalIF":3.3000,"publicationDate":"2024-04-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11057202/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAC-Antimicrobial Resistance","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jacamr/dlae028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: This study compared the performance of MIC test strip (ETEST), automated AST card (Vitek 2) and broth microdilution (BMD) in determining carbapenem susceptibility and MIC values of NDM-producing Enterobacterales.
Methods: NDM-producing Enterobacterales recovered from clinical specimens were included. The presence of blaNDM was confirmed by PCR. Identification of bacterial isolates was done by MALDI-TOF. Phenotypic susceptibility to three carbapenems (ertapenem, imipenem and meropenem) was tested by BMD, ETEST and Vitek 2. MIC values were interpreted in accordance with CLSI M100 (2022 edition). Using BMD as the reference standard, the essential agreement (EA), categorical agreement (CA), very major error (VME) and major error (ME) rates were evaluated.
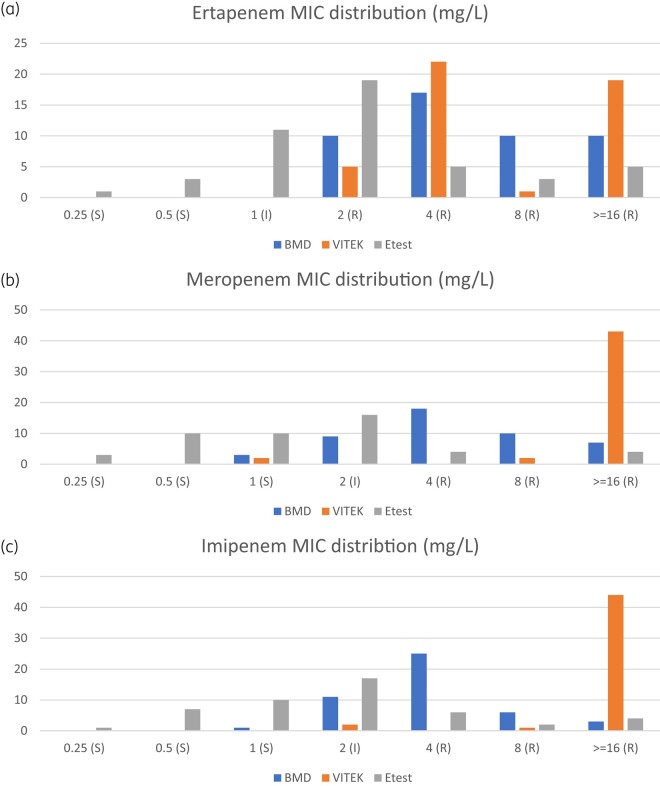
Results: Forty-seven NDM-producing Enterobacterales isolates were included, 44 of which were Escherichia coli. The EA of Vitek 2 was 97.9% for ertapenem, 25.5% for meropenem and 42.6% for imipenem. Using Vitek 2, there were 0% VMEs across all three carbapenems tested. The EA of ETEST was 53.2% for ertapenem, 55.3% for imipenem and 36.2% for meropenem. The rates of VMEs for ETEST were high too (ertapenem 8.5%, meropenem 36.2%, imipenem 26.1%). The MIC values obtained from Vitek 2 were consistently higher than those from BMD, while MICs from ETEST were consistently lower than those from BMD.
Conclusions: The VME rate for ETEST was unacceptably high when BMD was used as the standard for comparison. Vitek 2 had acceptable EA and CA for ertapenem when BMD was used as the standard for comparison. For meropenem and imipenem, neither of the methods (ETEST, Vitek 2) showed acceptable EA and CA when compared with BMD.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
