{"title":"Global trends in hepatitis C-related hepatocellular carcinoma mortality: A public database analysis (1999-2019).","authors":"Hassam Ali, Fnu Vikash, Vishali Moond, Fatima Khalid, Abdur Rehman Jamil, Dushyant Singh Dahiya, Amir Humza Sohail, Manesh Kumar Gangwani, Pratik Patel, Sanjaya K Satapathy","doi":"10.5501/wjv.v13.i1.89469","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hepatitis C is the leading cause of chronic liver disease worldwide and it significantly contributes to the burden of hepatocellular carcinoma (HCC). However, there are marked variations in the incidence and mortality rates of HCC across different geographical regions. With the advent of new widely available treatment modalities, such as direct-acting antivirals, it is becoming increasingly imperative to understand the temporal and geographical trends in HCC mortality associated with Hepatitis C. Furthermore, gender disparities in HCC mortality related to Hepatitis C are a crucial, yet underexplored aspect that adds to the disease's global impact. While some studies shed light on gender-specific trends, there is a lack of comprehensive data on global and regional mortality rates, particularly those highlighting gender disparities. This gap in knowledge hinders the development of targeted interventions and resource allocation strategies.</p><p><strong>Aim: </strong>To understand the global and regional trends in Hepatitis C-related HCC mortality rates from 1990 to 2019, along with gender disparities.</p><p><strong>Methods: </strong>We utilized the Global Burden of Disease database, a comprehensive repository for global health metrics to age-standardized mortality rates due to Hepatitis C-related HCC from 1999 to 2019. Rates were evaluated per 100000 population and assessed by World Bank-defined regions. Temporal trends were determined using Joinpoint software and the Average Annual Percent Change (AAPC) method, and results were reported with 95% confidence intervals (CI).</p><p><strong>Results: </strong>From 1990 to 2019, overall, there was a significant decline in HCC-related mortality rates with an AAPC of -0.80% (95%CI: -0.83 to -0.77). Females demonstrated a marked decrease in mortality with an AAPC of -1.06% (95%CI: -1.09 to -1.03), whereas the male cohort had a lower AAPC of -0.52% (95%CI: -0.55 to -0.48). Regionally, East Asia and the Pacific demonstrated a significant decline with an AAPC of -2.05% (95%CI: -2.10 to -2.00), whereas Europe and Central Asia observed an uptrend with an AAPC of 0.72% (95%CI: 0.69 to 0.74). Latin America and the Caribbean also showed an uptrend with an AAPC of 0.06% (95%CI: 0.02 to 0.11). In the Middle East and North Africa, the AAPC was non-significant at 0.02% (95%CI: -0.09 to 0.12). North America, in contrast, displayed a significant upward trend with an AAPC of 2.63% (95%CI: 2.57 to 2.67). South Asia (AAPC -0.22%, 95%CI: -0.26 to -0.16) and Sub-Saharan Africa (AAPC -0.14%, 95%CI: -0.15 to -0.12) trends significantly declined over the study period.</p><p><strong>Conclusion: </strong>Our study reports disparities in Hepatitis C-related HCC mortality between 1999 to 2019, both regionally and between genders. While East Asia and the Pacific regions showed a promising decline in mortality, North America has experienced a concerning rise in mortality. These regional variations highlight the need for healthcare policymakers and practitioners to tailor public health strategies and interventions. The data serves as a call to action, particularly for regions where mortality rates are not improving, emphasizing the necessity for a nuanced, region-specific approach to combat the global challenge of HCC secondary to Hepatitis C.</p>","PeriodicalId":61903,"journal":{"name":"世界病毒学杂志(英文版)","volume":"13 1","pages":"89469"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11008397/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界病毒学杂志(英文版)","FirstCategoryId":"1089","ListUrlMain":"https://doi.org/10.5501/wjv.v13.i1.89469","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hepatitis C is the leading cause of chronic liver disease worldwide and it significantly contributes to the burden of hepatocellular carcinoma (HCC). However, there are marked variations in the incidence and mortality rates of HCC across different geographical regions. With the advent of new widely available treatment modalities, such as direct-acting antivirals, it is becoming increasingly imperative to understand the temporal and geographical trends in HCC mortality associated with Hepatitis C. Furthermore, gender disparities in HCC mortality related to Hepatitis C are a crucial, yet underexplored aspect that adds to the disease's global impact. While some studies shed light on gender-specific trends, there is a lack of comprehensive data on global and regional mortality rates, particularly those highlighting gender disparities. This gap in knowledge hinders the development of targeted interventions and resource allocation strategies.
Aim: To understand the global and regional trends in Hepatitis C-related HCC mortality rates from 1990 to 2019, along with gender disparities.
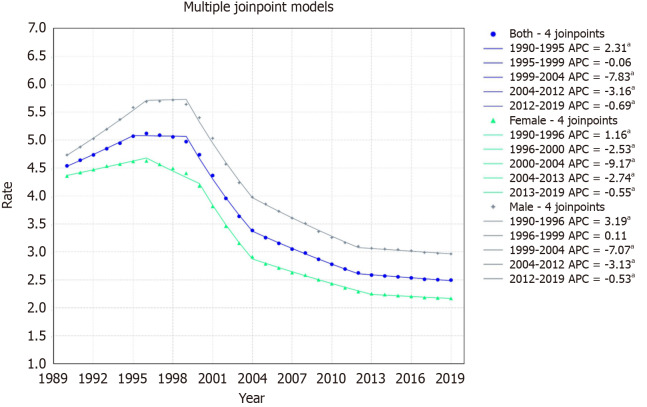
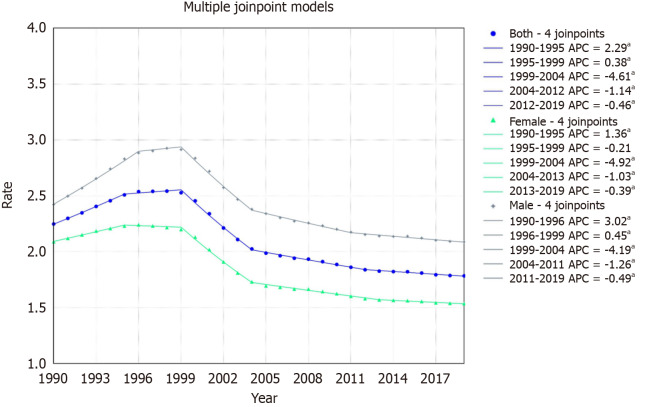
Methods: We utilized the Global Burden of Disease database, a comprehensive repository for global health metrics to age-standardized mortality rates due to Hepatitis C-related HCC from 1999 to 2019. Rates were evaluated per 100000 population and assessed by World Bank-defined regions. Temporal trends were determined using Joinpoint software and the Average Annual Percent Change (AAPC) method, and results were reported with 95% confidence intervals (CI).
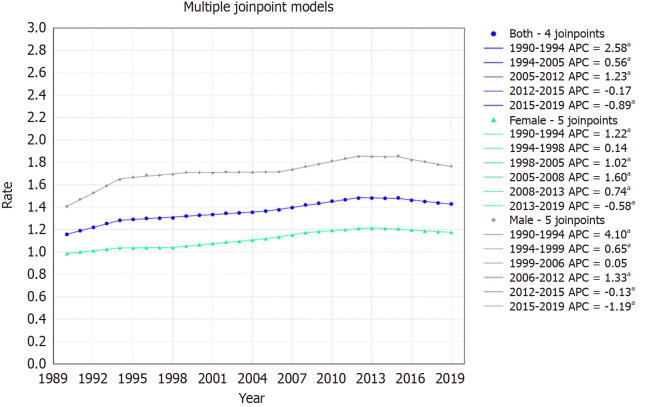
Results: From 1990 to 2019, overall, there was a significant decline in HCC-related mortality rates with an AAPC of -0.80% (95%CI: -0.83 to -0.77). Females demonstrated a marked decrease in mortality with an AAPC of -1.06% (95%CI: -1.09 to -1.03), whereas the male cohort had a lower AAPC of -0.52% (95%CI: -0.55 to -0.48). Regionally, East Asia and the Pacific demonstrated a significant decline with an AAPC of -2.05% (95%CI: -2.10 to -2.00), whereas Europe and Central Asia observed an uptrend with an AAPC of 0.72% (95%CI: 0.69 to 0.74). Latin America and the Caribbean also showed an uptrend with an AAPC of 0.06% (95%CI: 0.02 to 0.11). In the Middle East and North Africa, the AAPC was non-significant at 0.02% (95%CI: -0.09 to 0.12). North America, in contrast, displayed a significant upward trend with an AAPC of 2.63% (95%CI: 2.57 to 2.67). South Asia (AAPC -0.22%, 95%CI: -0.26 to -0.16) and Sub-Saharan Africa (AAPC -0.14%, 95%CI: -0.15 to -0.12) trends significantly declined over the study period.
Conclusion: Our study reports disparities in Hepatitis C-related HCC mortality between 1999 to 2019, both regionally and between genders. While East Asia and the Pacific regions showed a promising decline in mortality, North America has experienced a concerning rise in mortality. These regional variations highlight the need for healthcare policymakers and practitioners to tailor public health strategies and interventions. The data serves as a call to action, particularly for regions where mortality rates are not improving, emphasizing the necessity for a nuanced, region-specific approach to combat the global challenge of HCC secondary to Hepatitis C.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
