Pouria Motaghi, Iman Adibi, Peyman Adibi, Majid Ghasemi
{"title":"Small fiber neuropathy in irritable bowel syndrome.","authors":"Pouria Motaghi, Iman Adibi, Peyman Adibi, Majid Ghasemi","doi":"10.22037/ghfbb.v17i1.2827","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>In this study, we intend to evaluate the occurrence of small fiber neuropathy in patients with irritable bowel syndrome (IBS).</p><p><strong>Background: </strong>Small fiber neuropathy (SFN) is a sensory neuropathy that results from the degeneration of small Aδ and unmyelinated C fibers. SFN manifests positive symptoms, such as tingling, burning, prickling, and aching, and negative symptoms, including numbness, tightness, and coldness. The SFN coexistence with other comorbidities (e.g., fibromyalgia, inflammatory bowel disease, celiac disease) has been reported in previous studies.</p><p><strong>Methods: </strong>We conducted a cross-sectional study to assess the coexistence of SFN and IBS. Forty-two IBS patients and forty-three healthy individuals were asked to complete the Michigan Neuropathy Screening Instrument (MNSI) questionnaire. Results greater than three (>3) were considered positive. Participants with positive MNSI questionnaire results were examined for any neuropathy signs according to the Utah Early Neuropathy Scale (UENS) examination. The participants with positive results for the questionnaire and examination were checked for the sural and the superficial peroneal nerve conduction study (NCS). Normal NCS represented intact large fibers and the diagnosis of SFN.</p><p><strong>Results: </strong>Ten participants, 7 (16.7 %) in the IBS group and 3 (6.9 %) in the healthy group, had positive results for the questionnaire. Four participants were positive for the examination, with normal NCS, and were classified as SFN-positive. All four SFN diagnoses were from the IBS group. No one in the healthy group was diagnosed with SFN. We could find a significant statistical difference (p<0.05) between the IBS and healthy groups regarding the prevalence of SFN diagnosis.</p><p><strong>Conclusion: </strong>The co-occurrence of SFN and IBS suggests the possibility of a generalized neuropathy syndrome characterized by widespread neuronal impairment. Thus, any peripheral neuropathy symptom in IBS patients (and potentially other chronic pain disorders) should be evaluated for SFN since timely diagnosis and proper treatment result in a better quality of life for the patients.</p>","PeriodicalId":12636,"journal":{"name":"Gastroenterology and Hepatology From Bed to Bench","volume":"17 1","pages":"57-63"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11080693/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology and Hepatology From Bed to Bench","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/ghfbb.v17i1.2827","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: In this study, we intend to evaluate the occurrence of small fiber neuropathy in patients with irritable bowel syndrome (IBS).
Background: Small fiber neuropathy (SFN) is a sensory neuropathy that results from the degeneration of small Aδ and unmyelinated C fibers. SFN manifests positive symptoms, such as tingling, burning, prickling, and aching, and negative symptoms, including numbness, tightness, and coldness. The SFN coexistence with other comorbidities (e.g., fibromyalgia, inflammatory bowel disease, celiac disease) has been reported in previous studies.
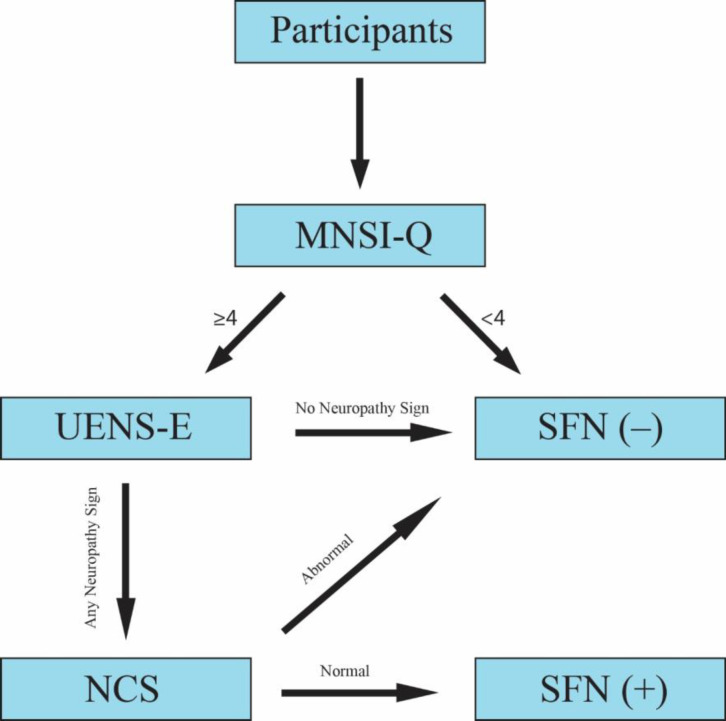
Methods: We conducted a cross-sectional study to assess the coexistence of SFN and IBS. Forty-two IBS patients and forty-three healthy individuals were asked to complete the Michigan Neuropathy Screening Instrument (MNSI) questionnaire. Results greater than three (>3) were considered positive. Participants with positive MNSI questionnaire results were examined for any neuropathy signs according to the Utah Early Neuropathy Scale (UENS) examination. The participants with positive results for the questionnaire and examination were checked for the sural and the superficial peroneal nerve conduction study (NCS). Normal NCS represented intact large fibers and the diagnosis of SFN.
Results: Ten participants, 7 (16.7 %) in the IBS group and 3 (6.9 %) in the healthy group, had positive results for the questionnaire. Four participants were positive for the examination, with normal NCS, and were classified as SFN-positive. All four SFN diagnoses were from the IBS group. No one in the healthy group was diagnosed with SFN. We could find a significant statistical difference (p<0.05) between the IBS and healthy groups regarding the prevalence of SFN diagnosis.
Conclusion: The co-occurrence of SFN and IBS suggests the possibility of a generalized neuropathy syndrome characterized by widespread neuronal impairment. Thus, any peripheral neuropathy symptom in IBS patients (and potentially other chronic pain disorders) should be evaluated for SFN since timely diagnosis and proper treatment result in a better quality of life for the patients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
