Kimberly M. Deininger, Heather D. Anderson, George P. Patrinos, Christina Mitropoulou, Christina L. Aquilante
{"title":"Cost-effectiveness analysis of CYP3A5 genotype-guided tacrolimus dosing in solid organ transplantation using real-world data","authors":"Kimberly M. Deininger, Heather D. Anderson, George P. Patrinos, Christina Mitropoulou, Christina L. Aquilante","doi":"10.1038/s41397-024-00334-1","DOIUrl":null,"url":null,"abstract":"The objective of this study was to estimate the cost-effectiveness of CYP3A5 genotype-guided tacrolimus dosing in kidney, liver, heart, and lung transplant recipients relative to standard of care (SOC) tacrolimus dosing, from a US healthcare payer perspective. We developed decision-tree models to compare economic and clinical outcomes between CYP3A5 genotype-guided and SOC tacrolimus therapy in the first six months post-transplant. We derived inputs for CYP3A5 phenotype frequencies and physician use of genotype test results to inform clinical care from literature; tacrolimus exposure [high vs low tacrolimus time in therapeutic range using the Rosendaal algorithm (TAC TTR-Rosendaal)] and outcomes (incidences of acute tacrolimus nephrotoxicity, acute cellular rejection, and death) from real-world data; and costs from the Medicare Fee Schedule and literature. We calculated cost per avoided event and performed sensitivity analyses to evaluate the robustness of the results to changes in inputs. Incremental costs per avoided event for CYP3A5 genotype-guided vs SOC tacrolimus dosing were $176,667 for kidney recipients, $364,000 for liver recipients, $12,982 for heart recipients, and $93,333 for lung recipients. The likelihood of CYP3A5 genotype-guided tacrolimus dosing leading to cost-savings was 19.8% in kidney, 32.3% in liver, 51.8% in heart, and 54.1% in lung transplant recipients. Physician use of genotype results to guide clinical care and the proportion of patients with a high TAC TTR-Rosendaal were key parameters driving the cost-effectiveness of CYP3A5 genotype-guided tacrolimus therapy. Relative to SOC, CYP3A5 genotype-guided tacrolimus dosing resulted in a slightly greater benefit at a higher cost. Further economic evaluations examining intermediary outcomes (e.g., dose modifications) are needed, particularly in populations with higher frequencies of CYP3A5 expressers.","PeriodicalId":54624,"journal":{"name":"Pharmacogenomics Journal","volume":"24 3","pages":"1-11"},"PeriodicalIF":2.9000,"publicationDate":"2024-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.nature.com/articles/s41397-024-00334-1.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacogenomics Journal","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41397-024-00334-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
Abstract
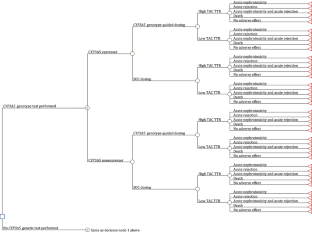
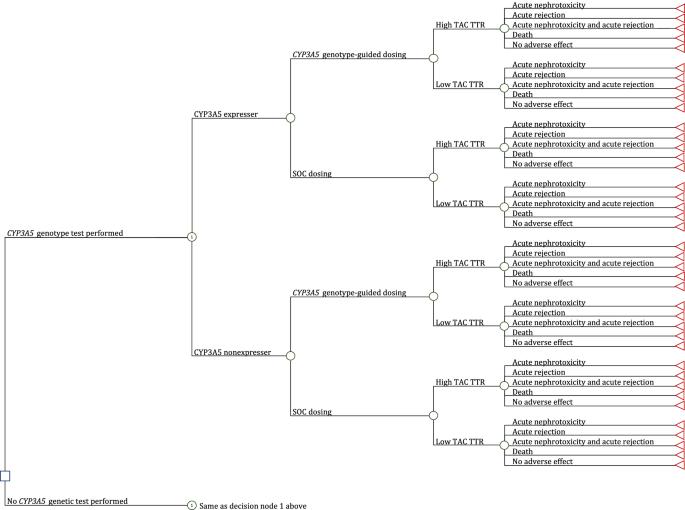
The objective of this study was to estimate the cost-effectiveness of CYP3A5 genotype-guided tacrolimus dosing in kidney, liver, heart, and lung transplant recipients relative to standard of care (SOC) tacrolimus dosing, from a US healthcare payer perspective. We developed decision-tree models to compare economic and clinical outcomes between CYP3A5 genotype-guided and SOC tacrolimus therapy in the first six months post-transplant. We derived inputs for CYP3A5 phenotype frequencies and physician use of genotype test results to inform clinical care from literature; tacrolimus exposure [high vs low tacrolimus time in therapeutic range using the Rosendaal algorithm (TAC TTR-Rosendaal)] and outcomes (incidences of acute tacrolimus nephrotoxicity, acute cellular rejection, and death) from real-world data; and costs from the Medicare Fee Schedule and literature. We calculated cost per avoided event and performed sensitivity analyses to evaluate the robustness of the results to changes in inputs. Incremental costs per avoided event for CYP3A5 genotype-guided vs SOC tacrolimus dosing were $176,667 for kidney recipients, $364,000 for liver recipients, $12,982 for heart recipients, and $93,333 for lung recipients. The likelihood of CYP3A5 genotype-guided tacrolimus dosing leading to cost-savings was 19.8% in kidney, 32.3% in liver, 51.8% in heart, and 54.1% in lung transplant recipients. Physician use of genotype results to guide clinical care and the proportion of patients with a high TAC TTR-Rosendaal were key parameters driving the cost-effectiveness of CYP3A5 genotype-guided tacrolimus therapy. Relative to SOC, CYP3A5 genotype-guided tacrolimus dosing resulted in a slightly greater benefit at a higher cost. Further economic evaluations examining intermediary outcomes (e.g., dose modifications) are needed, particularly in populations with higher frequencies of CYP3A5 expressers.
期刊介绍:
The Pharmacogenomics Journal is a print and electronic journal, which is dedicated to the rapid publication of original research on pharmacogenomics and its clinical applications.
Key areas of coverage include:
Personalized medicine
Effects of genetic variability on drug toxicity and efficacy
Identification and functional characterization of polymorphisms relevant to drug action
Pharmacodynamic and pharmacokinetic variations and drug efficacy
Integration of new developments in the genome project and proteomics into clinical medicine, pharmacology, and therapeutics
Clinical applications of genomic science
Identification of novel genomic targets for drug development
Potential benefits of pharmacogenomics.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
