Comparing and Evaluating the Role of Early Predictors Like BISAP and Ranson Scoring System with Modified CT Severity Index in Assessing the Severity of Acute Pancreatitis
{"title":"Comparing and Evaluating the Role of Early Predictors Like BISAP and Ranson Scoring System with Modified CT Severity Index in Assessing the Severity of Acute Pancreatitis","authors":"Raghav Gupta, Shyam Kumar Gupta","doi":"10.1007/s12262-024-04080-3","DOIUrl":null,"url":null,"abstract":"<p>Acute pancreatitis is a disorder characterized by acute necro-inflammatory changes of the pancreas and histologically marked by acinar cell destruction. It is one of the most common causes of hospitalization due to abdominal pain. Several classification systems have been proposed to assess the severity and prognosis of acute pancreatitis. Scores such as the Ranson and bedside index for severity in acute pancreatitis (BISAP) are useful for evaluating the severity and mortality of the disease. The revised Atlanta classification mainly focuses on the morphologic criteria for defining the various manifestations of acute pancreatitis outlined principally by means of CT and MRI. A case-series analysis study was conducted under the Department of Surgery, Government Medical College, Jammu, including 57 patients who presented with acute pancreatitis. The BISAP scores, along with Ranson scores and modified CT severity index scores (mCTSI), were calculated and compared using a preformed performa. The sensitivity, specificity, and area under the curve (AUC) of the BISAP and Ranson’s scoring systems were evaluated in patients who received CT scans, with mCTSI serving as the reference standard. The mean age of the study population was 46.49 years <i>SD</i> 14.11 with 14 (24.56%) men and 43 (75.44%) women. The men to women ratio was 0.32. Among the calculous etiology, cholelithiasis was the most common cause of acute pancreatitis, affecting 35 (61.40%) patients, followed by idiopathic acute pancreatitis. Out of 57 patients, 40 patients underwent CT scanning. Out of these 40 patients, 31 (77.5%) were classified as severe according to BISAP score with a cutoff of BISAP score ≥ 2, and 33 (82.5%) were classified as severe according to Ranson scoring system, with a cutoff of Ranson score ≥ 3. The sensitivity and specificity of BISAP were 90.90% and 85.71%, respectively. The sensitivity and specificity of Ranson were 93.93% and 71.42%, respectively. Ranson was more sensitive but less specific than BISAP. In our study, area under curve (AUC) of BISAP was 0.70, and area under curve (AUC) of Ranson was 0.94. Ranson scoring was more accurate than BISAP in predicting severe acute pancreatitis, according to area under curve (AUC). BISAP scoring is comparable to the Ranson score in predicting the severity of acute pancreatitis, with statistically insignificant <i>p</i>-value (<i>p</i> = 0.089). The bedside index for severity in acute pancreatitis (BISAP) offers a straightforward and timely means of identifying severe cases within 24 h of disease onset. Conversely, Ranson’s score retains its value in pinpointing patients at risk of severe acute pancreatitis and ensuing organ failure. In our study, <i>p</i>-value is > 0.05, which indicates that both BISAP and Ranson’s score are equally adept at assessing acute pancreatitis severity, serving as reliable prognostic tools for early patient intervention. However, Ranson’s score boasts superior sensitivity and specificity compared to BISAP, reinforcing its utility in clinical practice.</p>","PeriodicalId":13391,"journal":{"name":"Indian Journal of Surgery","volume":"1 1","pages":""},"PeriodicalIF":0.4000,"publicationDate":"2024-05-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12262-024-04080-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
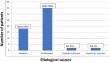
Acute pancreatitis is a disorder characterized by acute necro-inflammatory changes of the pancreas and histologically marked by acinar cell destruction. It is one of the most common causes of hospitalization due to abdominal pain. Several classification systems have been proposed to assess the severity and prognosis of acute pancreatitis. Scores such as the Ranson and bedside index for severity in acute pancreatitis (BISAP) are useful for evaluating the severity and mortality of the disease. The revised Atlanta classification mainly focuses on the morphologic criteria for defining the various manifestations of acute pancreatitis outlined principally by means of CT and MRI. A case-series analysis study was conducted under the Department of Surgery, Government Medical College, Jammu, including 57 patients who presented with acute pancreatitis. The BISAP scores, along with Ranson scores and modified CT severity index scores (mCTSI), were calculated and compared using a preformed performa. The sensitivity, specificity, and area under the curve (AUC) of the BISAP and Ranson’s scoring systems were evaluated in patients who received CT scans, with mCTSI serving as the reference standard. The mean age of the study population was 46.49 years SD 14.11 with 14 (24.56%) men and 43 (75.44%) women. The men to women ratio was 0.32. Among the calculous etiology, cholelithiasis was the most common cause of acute pancreatitis, affecting 35 (61.40%) patients, followed by idiopathic acute pancreatitis. Out of 57 patients, 40 patients underwent CT scanning. Out of these 40 patients, 31 (77.5%) were classified as severe according to BISAP score with a cutoff of BISAP score ≥ 2, and 33 (82.5%) were classified as severe according to Ranson scoring system, with a cutoff of Ranson score ≥ 3. The sensitivity and specificity of BISAP were 90.90% and 85.71%, respectively. The sensitivity and specificity of Ranson were 93.93% and 71.42%, respectively. Ranson was more sensitive but less specific than BISAP. In our study, area under curve (AUC) of BISAP was 0.70, and area under curve (AUC) of Ranson was 0.94. Ranson scoring was more accurate than BISAP in predicting severe acute pancreatitis, according to area under curve (AUC). BISAP scoring is comparable to the Ranson score in predicting the severity of acute pancreatitis, with statistically insignificant p-value (p = 0.089). The bedside index for severity in acute pancreatitis (BISAP) offers a straightforward and timely means of identifying severe cases within 24 h of disease onset. Conversely, Ranson’s score retains its value in pinpointing patients at risk of severe acute pancreatitis and ensuing organ failure. In our study, p-value is > 0.05, which indicates that both BISAP and Ranson’s score are equally adept at assessing acute pancreatitis severity, serving as reliable prognostic tools for early patient intervention. However, Ranson’s score boasts superior sensitivity and specificity compared to BISAP, reinforcing its utility in clinical practice.
期刊介绍:
The Indian Journal of Surgery is the official publication of the Association of Surgeons of India that considers for publication articles in all fields of surgery. Issues are published bimonthly in the months of February, April, June, August, October and December.
The journal publishes Original article, Point of technique, Review article, Case report, Letter to editor, Teachers and surgeons from the past - A short (up to 500 words) bio sketch of a revered teacher or surgeon whom you hold in esteem and Images in surgery, surgical pathology, and surgical radiology.
A trusted resource for peer-reviewed coverage of all types of surgery
Provides a forum for surgeons in India and abroad to exchange ideas and advance the art of surgery
The official publication of the Association of Surgeons of India
92% of authors who answered a survey reported that they would definitely publish or probably publish in the journal again
The Indian Journal of Surgery offers peer-reviewed coverage of all types of surgery. The Journal publishes Original articles, Points of technique, Review articles, Case reports, Letters, Images and brief biographies of influential teachers and surgeons.
The Journal spans General Surgery, Pediatric Surgery, Neurosurgery, Plastic Surgery, Cardiothoracic Surgery, Vascular Surgery, Rural Surgery, Orthopedic Surgery, Urology, Surgical Oncology, Radiology, Anaesthesia, Trauma Services, Minimal Access Surgery, Endocrine Surgery, GI Surgery, ENT, Colorectal Surgery, surgical practice and research.
The Journal provides a forum for surgeons from India and abroad to exchange ideas, to propagate the advancement of science and the art of surgery and to promote friendship among surgeons in India and abroad. This has been a trusted platform for surgons in communicating up-to-date scientific informeation to the community.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
