Pascale J King, Lana Ramic, Janet Wilson, Shawn Aaron, Ian G Stiell
{"title":"Evaluation of the quality of emergency department management for patients with chronic obstructive pulmonary disease.","authors":"Pascale J King, Lana Ramic, Janet Wilson, Shawn Aaron, Ian G Stiell","doi":"10.15441/ceem.24.197","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Chronic obstructive pulmonary disease (COPD) is associated with exacerbations and high risk of serious outcomes. Our goal was to determine the appropriateness of the emergency department (ED) management of COPD exacerbations.</p><p><strong>Methods: </strong>This observational cohort study incorporated a health records review and included COPD exacerbation cases seen at two large academic EDs. We included all patients with the primary diagnosis of COPD exacerbation. From the electronic medical record, demographic and clinical data were abstracted, and the Ottawa COPD Risk Score (OCRS) was calculated for each. Short-term serious outcomes included intensive care unit admission, intubation, myocardial infarction, noninvasive positive pressure ventilation (NIV), and death at 30 days. Cases were judged for appropriateness of treatment according to explicit indications and standards developed a priori.</p><p><strong>Results: </strong>We enrolled 500 cases with mean age of 71.9 years, 51.2% female patients, 50.2% admitted, and 4.4% death. The calculated OCRS score was >2 for 70.8% of patients. The treatments provided were inhaled β-agonists (82.6%), inhaled anticholinergics (76.6%), corticosteroids (75.2%), antibiotics (71.0%), oxygen (63.8%), NIV (8.8%), and intubation (0.6%). Overall, 50.0% of cases were judged to have had inadequate management due to missing treatments. Specifically, the proportion of missing treatments were inhaled β-agonist (17.0%), inhaled anticholinergic (22.6%), corticosteroids (24.4%), antibiotics (12.8%), and NIV (2.0%).</p><p><strong>Conclusion: </strong>Adequate treatment of COPD exacerbation was lacking in 50.0% of patients in these two large academic EDs. Concerning were the number of patients not receiving corticosteroids or antibiotics. Implementation of explicit treatment standards should lead to improved patient care of this common and serious condition.</p>","PeriodicalId":10325,"journal":{"name":"Clinical and Experimental Emergency Medicine","volume":" ","pages":"268-275"},"PeriodicalIF":2.3000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11467456/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15441/ceem.24.197","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/23 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Chronic obstructive pulmonary disease (COPD) is associated with exacerbations and high risk of serious outcomes. Our goal was to determine the appropriateness of the emergency department (ED) management of COPD exacerbations.
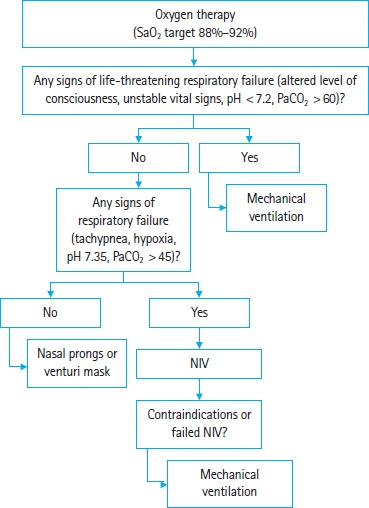
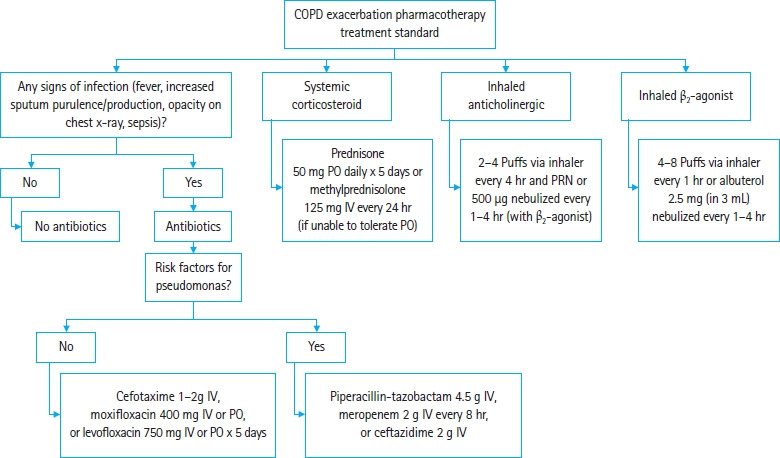
Methods: This observational cohort study incorporated a health records review and included COPD exacerbation cases seen at two large academic EDs. We included all patients with the primary diagnosis of COPD exacerbation. From the electronic medical record, demographic and clinical data were abstracted, and the Ottawa COPD Risk Score (OCRS) was calculated for each. Short-term serious outcomes included intensive care unit admission, intubation, myocardial infarction, noninvasive positive pressure ventilation (NIV), and death at 30 days. Cases were judged for appropriateness of treatment according to explicit indications and standards developed a priori.
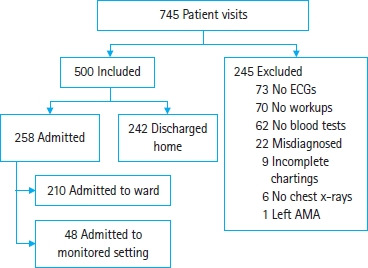
Results: We enrolled 500 cases with mean age of 71.9 years, 51.2% female patients, 50.2% admitted, and 4.4% death. The calculated OCRS score was >2 for 70.8% of patients. The treatments provided were inhaled β-agonists (82.6%), inhaled anticholinergics (76.6%), corticosteroids (75.2%), antibiotics (71.0%), oxygen (63.8%), NIV (8.8%), and intubation (0.6%). Overall, 50.0% of cases were judged to have had inadequate management due to missing treatments. Specifically, the proportion of missing treatments were inhaled β-agonist (17.0%), inhaled anticholinergic (22.6%), corticosteroids (24.4%), antibiotics (12.8%), and NIV (2.0%).
Conclusion: Adequate treatment of COPD exacerbation was lacking in 50.0% of patients in these two large academic EDs. Concerning were the number of patients not receiving corticosteroids or antibiotics. Implementation of explicit treatment standards should lead to improved patient care of this common and serious condition.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
