Jaleh Aghaie, Marianne Lisby, Marie Kristine Jessen
{"title":"Physician awareness of fluid volume administered with intravenous antibiotics: a structured interview-based study.","authors":"Jaleh Aghaie, Marianne Lisby, Marie Kristine Jessen","doi":"10.15441/ceem.24.219","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Fluids administered as drug diluents with intravenous (IV) medicine constitute a substantial fraction of fluids in inpatients. Whether physicians are aware of fluid volumes administered with IV antibiotics for patients with suspected infections is unclear. Moreover, whether this leads to adjustments in 24-hour fluid administration/antibiotics is unknown.</p><p><strong>Methods: </strong>This cross-sectional interview-based study was conducted in three emergency departments. Physicians were interviewed after prescribing around-the-clock IV antibiotics for ≥24 hours to patients with suspected infection. A structured interview guide assessed the physicians' awareness, considerations, and practices when prescribing IV antibiotics. The 24-hour antibiotic fluid volume was calculated.</p><p><strong>Results: </strong>We interviewed 100 physicians. The 24-hour fluid volume administered with IV antibiotics was 400 mL (interquartile range, 300-400 mL). Overall, 53 physicians (53%) were unaware of the fluid volume administered with IV antibiotics. Moreover, 76 (76%) did not account for the antibiotic fluid volume in the 24-hour fluid administration, and 96 (96%) indicated that they would not adjust prescribed fluids after receiving information about 24-hour antibiotic fluid volume administered for their patient. No comorbidities associated with fluid intolerance were the primary reason for not adjusting prescribed fluids/ antibiotics. Approximately 79 (79%) opted for visibility of fluid volumes administered with IV antibiotics in the medical record.</p><p><strong>Conclusion: </strong>The majority of physicians were unaware of fluid volumes administered as a drug diluent with IV antibiotics. The majority chose not to make post-prescribing adjustments to their planned fluid administration; they regarded their patient as fluid tolerant. The physicians opted for visibility of fluid volumes administered as diluents during the prescribing process.</p>","PeriodicalId":10325,"journal":{"name":"Clinical and Experimental Emergency Medicine","volume":" ","pages":"66-75"},"PeriodicalIF":2.3000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12010794/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15441/ceem.24.219","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/23 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Fluids administered as drug diluents with intravenous (IV) medicine constitute a substantial fraction of fluids in inpatients. Whether physicians are aware of fluid volumes administered with IV antibiotics for patients with suspected infections is unclear. Moreover, whether this leads to adjustments in 24-hour fluid administration/antibiotics is unknown.
Methods: This cross-sectional interview-based study was conducted in three emergency departments. Physicians were interviewed after prescribing around-the-clock IV antibiotics for ≥24 hours to patients with suspected infection. A structured interview guide assessed the physicians' awareness, considerations, and practices when prescribing IV antibiotics. The 24-hour antibiotic fluid volume was calculated.
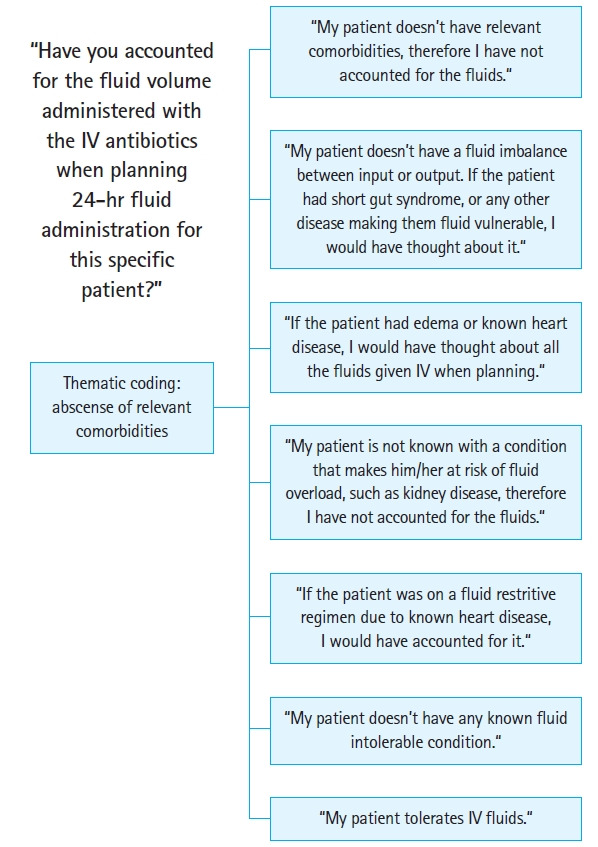
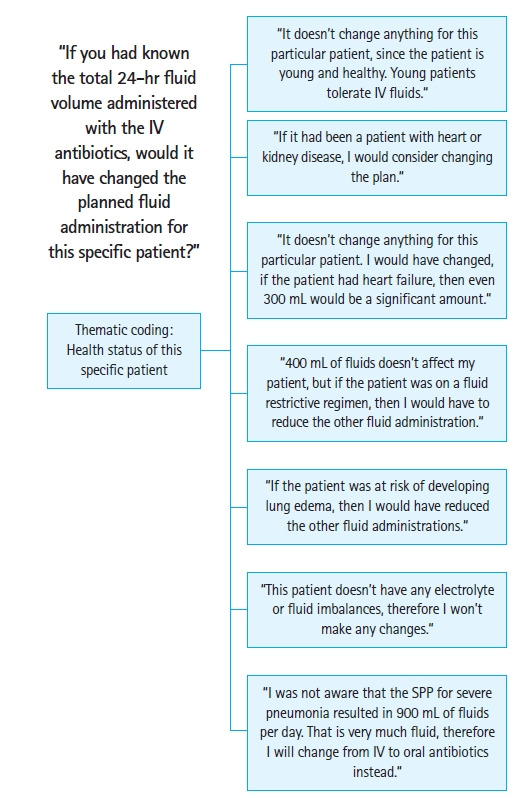
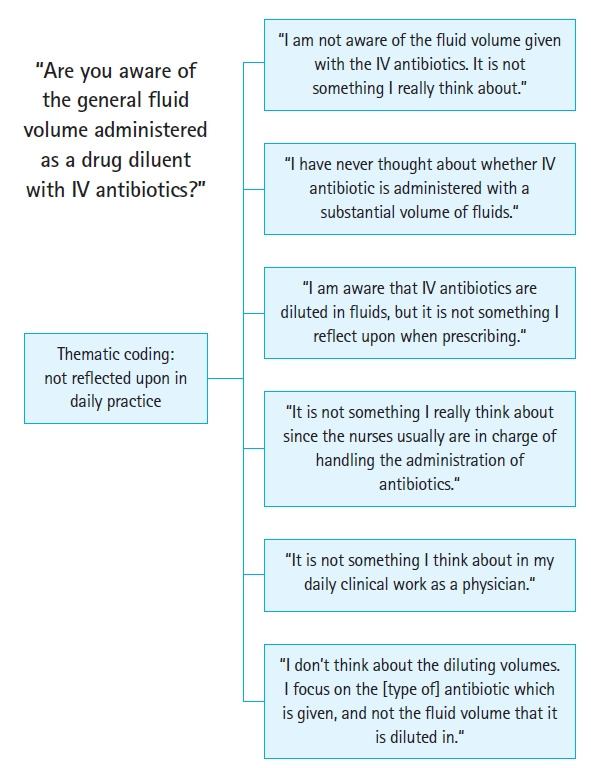
Results: We interviewed 100 physicians. The 24-hour fluid volume administered with IV antibiotics was 400 mL (interquartile range, 300-400 mL). Overall, 53 physicians (53%) were unaware of the fluid volume administered with IV antibiotics. Moreover, 76 (76%) did not account for the antibiotic fluid volume in the 24-hour fluid administration, and 96 (96%) indicated that they would not adjust prescribed fluids after receiving information about 24-hour antibiotic fluid volume administered for their patient. No comorbidities associated with fluid intolerance were the primary reason for not adjusting prescribed fluids/ antibiotics. Approximately 79 (79%) opted for visibility of fluid volumes administered with IV antibiotics in the medical record.
Conclusion: The majority of physicians were unaware of fluid volumes administered as a drug diluent with IV antibiotics. The majority chose not to make post-prescribing adjustments to their planned fluid administration; they regarded their patient as fluid tolerant. The physicians opted for visibility of fluid volumes administered as diluents during the prescribing process.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
