Abdullah K Malik, Samuel J Tingle, Chris Varghese, Ruth Owen, Balaji Mahendran, Rodrigo Figueiredo, Aimen O Amer, Ian S Currie, Steven A White, Derek M Manas, Colin H Wilson
{"title":"Does Time to Asystole in Donors After Circulatory Death Impact Recipient Outcome in Liver Transplantation?","authors":"Abdullah K Malik, Samuel J Tingle, Chris Varghese, Ruth Owen, Balaji Mahendran, Rodrigo Figueiredo, Aimen O Amer, Ian S Currie, Steven A White, Derek M Manas, Colin H Wilson","doi":"10.1097/TP.0000000000005074","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The agonal phase can vary following treatment withdrawal in donor after circulatory death (DCD). There is little evidence to support when procurement teams should stand down in relation to donor time to death (TTD). We assessed what impact TTD had on outcomes following DCD liver transplantation.</p><p><strong>Methods: </strong>Data were extracted from the UK Transplant Registry on DCD liver transplant recipients from 2006 to 2021. TTD was the time from withdrawal of life-sustaining treatment to asystole, and functional warm ischemia time was the time from donor systolic blood pressure and/or oxygen saturation falling below 50 mm Hg and 70%, respectively, to aortic perfusion. The primary endpoint was 1-y graft survival. Potential predictors were fitted into Cox proportional hazards models. Adjusted restricted cubic spline models were generated to further delineate the relationship between TTD and outcome.</p><p><strong>Results: </strong>One thousand five hundred fifty-eight recipients of a DCD liver graft were included. Median TTD in the entire cohort was 13 min (interquartile range, 9-17 min). Restricted cubic splines revealed that the risk of graft loss was significantly greater when TTD ≤14 min. After 14 min, there was no impact on graft loss. Prolonged hepatectomy time was significantly associated with graft loss (hazard ratio, 1.87; 95% confidence interval, 1.23-2.83; P = 0.003); however, functional warm ischemia time had no impact (hazard ratio, 1.00; 95% confidence interval, 0.44-2.27; P > 0.9).</p><p><strong>Conclusions: </strong>A very short TTD was associated with increased risk of graft loss, possibly because of such donors being more unstable and/or experiencing brain stem death as well as circulatory death. Expanding the stand down times may increase the utilization of donor livers without significantly impairing graft outcome.</p>","PeriodicalId":23316,"journal":{"name":"Transplantation","volume":" ","pages":"2238-2246"},"PeriodicalIF":5.0000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11495538/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/TP.0000000000005074","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The agonal phase can vary following treatment withdrawal in donor after circulatory death (DCD). There is little evidence to support when procurement teams should stand down in relation to donor time to death (TTD). We assessed what impact TTD had on outcomes following DCD liver transplantation.
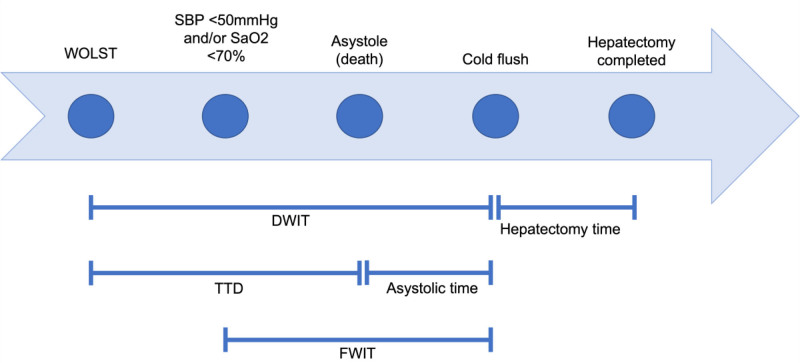
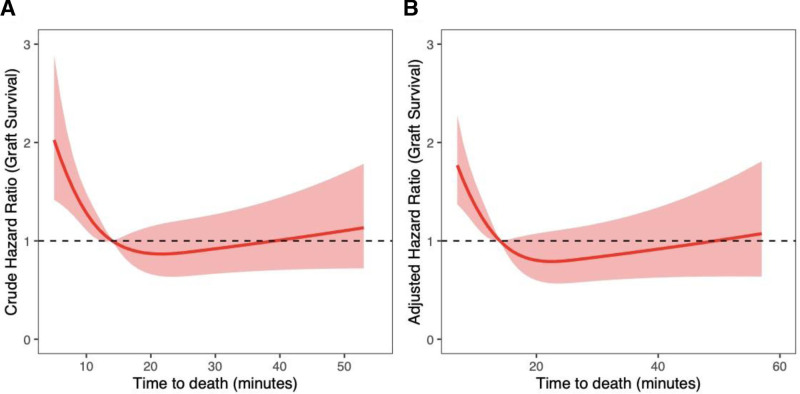
Methods: Data were extracted from the UK Transplant Registry on DCD liver transplant recipients from 2006 to 2021. TTD was the time from withdrawal of life-sustaining treatment to asystole, and functional warm ischemia time was the time from donor systolic blood pressure and/or oxygen saturation falling below 50 mm Hg and 70%, respectively, to aortic perfusion. The primary endpoint was 1-y graft survival. Potential predictors were fitted into Cox proportional hazards models. Adjusted restricted cubic spline models were generated to further delineate the relationship between TTD and outcome.
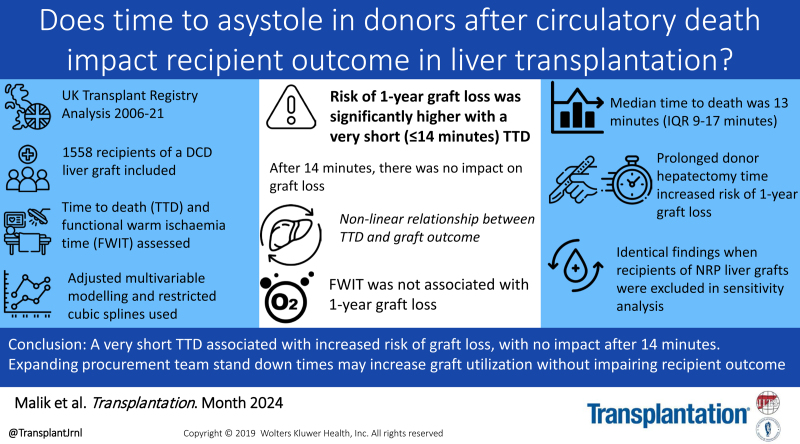
Results: One thousand five hundred fifty-eight recipients of a DCD liver graft were included. Median TTD in the entire cohort was 13 min (interquartile range, 9-17 min). Restricted cubic splines revealed that the risk of graft loss was significantly greater when TTD ≤14 min. After 14 min, there was no impact on graft loss. Prolonged hepatectomy time was significantly associated with graft loss (hazard ratio, 1.87; 95% confidence interval, 1.23-2.83; P = 0.003); however, functional warm ischemia time had no impact (hazard ratio, 1.00; 95% confidence interval, 0.44-2.27; P > 0.9).
Conclusions: A very short TTD was associated with increased risk of graft loss, possibly because of such donors being more unstable and/or experiencing brain stem death as well as circulatory death. Expanding the stand down times may increase the utilization of donor livers without significantly impairing graft outcome.
期刊介绍:
The official journal of The Transplantation Society, and the International Liver Transplantation Society, Transplantation is published monthly and is the most cited and influential journal in the field, with more than 25,000 citations per year.
Transplantation has been the trusted source for extensive and timely coverage of the most important advances in transplantation for over 50 years. The Editors and Editorial Board are an international group of research and clinical leaders that includes many pioneers of the field, representing a diverse range of areas of expertise. This capable editorial team provides thoughtful and thorough peer review, and delivers rapid, careful and insightful editorial evaluation of all manuscripts submitted to the journal.
Transplantation is committed to rapid review and publication. The journal remains competitive with a time to first decision of fewer than 21 days. Transplantation was the first in the field to offer CME credit to its peer reviewers for reviews completed.
The journal publishes original research articles in original clinical science and original basic science. Short reports bring attention to research at the forefront of the field. Other areas covered include cell therapy and islet transplantation, immunobiology and genomics, and xenotransplantation.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
