{"title":"Surgical treatment for recurrent thoracic ventral intradural arachnoid cyst secondary to tuberculous meningitis: a case report.","authors":"Yushi Sakamoto, Takayoshi Shimizu, Bungo Otsuki, Shuichi Matsuda","doi":"10.1038/s41394-024-00650-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Spinal intradural arachnoid cysts (SIACs) are rare spinal entities that are categorized as primary or secondary pathologies. Secondary cysts can arise from various traumatic or inflammatory causes including subarachnoid hemorrhage, intrathecal injection or surgery, and infectious meningitis/arachnoiditis. Only a few cases of SIAC secondary to tuberculous meningitis have been previously reported, without details of the surgical treatment.</p><p><strong>Case presentation: </strong>A 27-year-old woman diagnosed with tuberculous meningitis developed myelopathy caused by thoracic ventral SIAC and intradural abscess. The patient underwent abscess evacuation and cyst fenestration; however, cyst recurrence occurred. The 2nd surgery consisted of cyst resection via a posterolateral approach with expansive duraplasty and spinal arthrodesis. Re-recurrence occurred, and at the 3rd surgery, cyst-subarachnoid bypass was performed. One year after the 3rd surgery, the myelopathic symptoms recovered, and MR images demonstrated a decreased cyst size.</p><p><strong>Discussion: </strong>Here, we report a rare case of recurrent thoracic SIAC secondary to tuberculous meningitis and arachnoiditis. Simple fenestration is associated with a high risk of recurrence in this pathology. Ventrally located thoracic cysts can be approached with posterolateral approach with pedicles resected followed by instrumented arthrodesis. Even in cases involving gross total resection of the cyst wall, there is a risk of recurrence. In such cases, cyst-subarachnoid bypass with a large-diameter tube can be effective.</p>","PeriodicalId":22079,"journal":{"name":"Spinal Cord Series and Cases","volume":"10 1","pages":"36"},"PeriodicalIF":0.9000,"publicationDate":"2024-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11116473/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spinal Cord Series and Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s41394-024-00650-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Spinal intradural arachnoid cysts (SIACs) are rare spinal entities that are categorized as primary or secondary pathologies. Secondary cysts can arise from various traumatic or inflammatory causes including subarachnoid hemorrhage, intrathecal injection or surgery, and infectious meningitis/arachnoiditis. Only a few cases of SIAC secondary to tuberculous meningitis have been previously reported, without details of the surgical treatment.
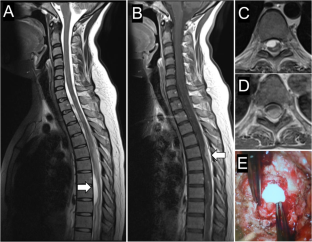
Case presentation: A 27-year-old woman diagnosed with tuberculous meningitis developed myelopathy caused by thoracic ventral SIAC and intradural abscess. The patient underwent abscess evacuation and cyst fenestration; however, cyst recurrence occurred. The 2nd surgery consisted of cyst resection via a posterolateral approach with expansive duraplasty and spinal arthrodesis. Re-recurrence occurred, and at the 3rd surgery, cyst-subarachnoid bypass was performed. One year after the 3rd surgery, the myelopathic symptoms recovered, and MR images demonstrated a decreased cyst size.
Discussion: Here, we report a rare case of recurrent thoracic SIAC secondary to tuberculous meningitis and arachnoiditis. Simple fenestration is associated with a high risk of recurrence in this pathology. Ventrally located thoracic cysts can be approached with posterolateral approach with pedicles resected followed by instrumented arthrodesis. Even in cases involving gross total resection of the cyst wall, there is a risk of recurrence. In such cases, cyst-subarachnoid bypass with a large-diameter tube can be effective.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
