Leigh C Johnston, Patrick Ngassa Piotie, Innocent Maposa, Sandhya Singh, Lazarus Kuonza, Alex De Voux
{"title":"Determinants of sub-optimal glycemic control among patients enrolled in a medicine dispensing programme in KwaZulu-Natal: A cohort study, 2018-2021.","authors":"Leigh C Johnston, Patrick Ngassa Piotie, Innocent Maposa, Sandhya Singh, Lazarus Kuonza, Alex De Voux","doi":"10.4102/phcfm.v16i1.4336","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong> The Central Chronic Medicines Dispensing and Distribution (CCMDD) programme facilitates clinically stable patients to collect their chronic medication from community-based pick-up points.</p><p><strong>Aim: </strong> We determined baseline glycaemic control and rates and predictors of becoming sub-optimally controlled for type 2 diabetes mellitus (T2DM) CCMDD-enrolled patients.</p><p><strong>Setting: </strong> The setting of the study was eThekwini, KwaZulu-Natal, South Africa.</p><p><strong>Methods: </strong> We performed a cohort study (April 2018- December 2021). We linked T2DM CCMDD-enrolled patients to glycated haemoglobin (HbA1c) data from the National Health Laboratory Service. We selected patients optimally controlled at their baseline HbA1c, with ≥ 1 repeat-test available. We used Kaplan-Meier analysis to assess survival rates and extended Cox regression to determine associations between time to sub-optimal control (HbA1c 7%) and predictors. Adjusted hazard ratios (aHRs), 95% confidence interval (CI), and p-values are reported.</p><p><strong>Results: </strong> Of the 41145 T2DM patients enrolled in the CCMDD programme, 7960 (19%) had a HbA1c result available. Twenty-seven percent (2147/7960) were optimally controlled at their baseline HbA1c. Of those controlled at baseline, 695 (32%) patients had a repeat test available, with 35% (242/695) changing to sub-optimal status. The HbA1c testing frequency as per national guidelines was associated with a lower hazard of sub-optimal glycaemic control (aHR: 0.46; 95% CI: 0.24-0.91; p-value = 0.024). Patients prescribed dual-therapy had a higher hazard of sub-optimal glycaemic control (aHR: 1.50; 95% CI: 1.16-1.95; p-value = 0.002) versus monotherapy.</p><p><strong>Conclusions: </strong> The HbA1c monitoring, in-line with testing frequency guidelines, is needed to alert the CCMDD programme of patients who become ineligible for enrolment. Patients receiving dual-therapy require special consideration.Contribution: Addressing identified shortfalls can assist programme implementation.</p>","PeriodicalId":47037,"journal":{"name":"African Journal of Primary Health Care & Family Medicine","volume":"16 1","pages":"e1-e12"},"PeriodicalIF":1.7000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11151363/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"African Journal of Primary Health Care & Family Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/phcfm.v16i1.4336","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Central Chronic Medicines Dispensing and Distribution (CCMDD) programme facilitates clinically stable patients to collect their chronic medication from community-based pick-up points.
Aim: We determined baseline glycaemic control and rates and predictors of becoming sub-optimally controlled for type 2 diabetes mellitus (T2DM) CCMDD-enrolled patients.
Setting: The setting of the study was eThekwini, KwaZulu-Natal, South Africa.
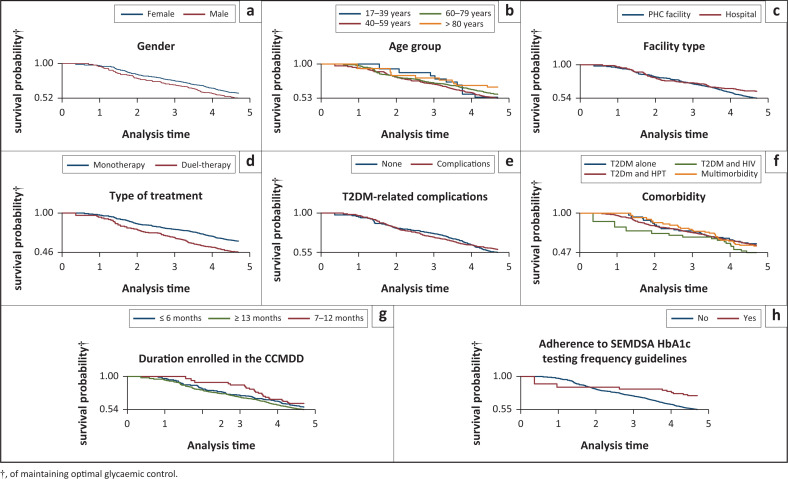
Methods: We performed a cohort study (April 2018- December 2021). We linked T2DM CCMDD-enrolled patients to glycated haemoglobin (HbA1c) data from the National Health Laboratory Service. We selected patients optimally controlled at their baseline HbA1c, with ≥ 1 repeat-test available. We used Kaplan-Meier analysis to assess survival rates and extended Cox regression to determine associations between time to sub-optimal control (HbA1c 7%) and predictors. Adjusted hazard ratios (aHRs), 95% confidence interval (CI), and p-values are reported.
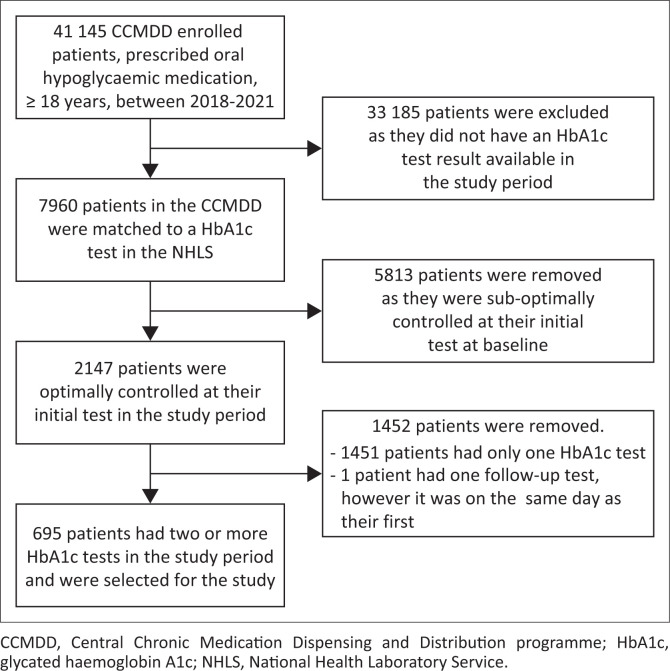
Results: Of the 41145 T2DM patients enrolled in the CCMDD programme, 7960 (19%) had a HbA1c result available. Twenty-seven percent (2147/7960) were optimally controlled at their baseline HbA1c. Of those controlled at baseline, 695 (32%) patients had a repeat test available, with 35% (242/695) changing to sub-optimal status. The HbA1c testing frequency as per national guidelines was associated with a lower hazard of sub-optimal glycaemic control (aHR: 0.46; 95% CI: 0.24-0.91; p-value = 0.024). Patients prescribed dual-therapy had a higher hazard of sub-optimal glycaemic control (aHR: 1.50; 95% CI: 1.16-1.95; p-value = 0.002) versus monotherapy.
Conclusions: The HbA1c monitoring, in-line with testing frequency guidelines, is needed to alert the CCMDD programme of patients who become ineligible for enrolment. Patients receiving dual-therapy require special consideration.Contribution: Addressing identified shortfalls can assist programme implementation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
