
Debate continues as to the optimum hemodialysis (HD) dialysate calcium concentration. Although current guidelines advocate 1.25–1.5 mmol/L, some investigators have suggested these may cause calcium gains. As such we investigated whether using dialysate calcium of 1.25 mmol/L risked calcium gains, and whether there were differences between hemodiafiltration and high flux HD.
We continuously collect an aliquot of effluent dialysate during dialysis sessions, and calculated dialysis calcium mass balance by the difference between the amount of calcium delivered as fresh dialysate and that lost in effluent dialysate.
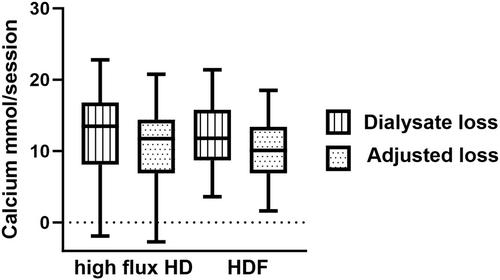
We studied 106 stable outpatients, 64% male, mean age 64.4 ± 16.2 years, median dialysis vintage 32 (22–60) months. Most sessions (69%) used a 1.0 mmol/L calcium dialysate, with a median sessional loss of 13.7 (11.5–17.1) mmol, whereas using 1.25 mmol/L the median loss was 7.4 (4.9–10.1) mmol, but with 6.9% had a positive balance (p = 0.031 vs dialysate calcium 1.0 mmol/L). Most patients (85.8%) were treated by hemodiafiltration, but there was no difference in sessional losses (11.7 (8.4–15.8) vs 13.5 (8.1–16.8)) with high flux HD. Dialysis sessional calcium balance was associated with the use of lower dialysate calcium concentration (β −19.5, 95% confidence limits (95%CL) −27.7 to −11.3, p < 0.001), and sessional duration (β 0.07 (95% CL) 0.03–012, p = 0.002).
Ideally, the choice of dialysate calcium should be individualized, but clinicians should be aware, that even when using a dialysate calcium of 1.25 mmol/L, some patients are at risk of a calcium gain during hemodiafiltration and high-flux hemodialysis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
