Christof Kaltenmeier, Hao Liu, Xingyu Zhang, Armando Ganoza, Andrew Crane, Colin Powers, Vikraman Gunabushanam, Jaideep Behari, Michele Molinari
{"title":"Survival after live donor versus deceased donor liver transplantation: propensity score-matched study.","authors":"Christof Kaltenmeier, Hao Liu, Xingyu Zhang, Armando Ganoza, Andrew Crane, Colin Powers, Vikraman Gunabushanam, Jaideep Behari, Michele Molinari","doi":"10.1093/bjsopen/zrae058","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>For individuals with advanced liver disease, equipoise in outcomes between live donor liver transplant (LDLT) and deceased donor liver transplant (DDLT) is uncertain.</p><p><strong>Methods: </strong>A retrospective cohort study was performed using data extracted from the Scientific Registry of Transplant Recipients. Adults who underwent first-time DDLT or LTDL in the United States between 2002 and 2020 were paired using propensity-score matching with 1:10 ratio without replacement. Patient and graft survival were compared using the model for end-stage liver disease (MELD) score for stratification.</p><p><strong>Results: </strong>After propensity-score matching, 31 522 DDLT and 3854 LDLT recipients were included. For recipients with MELD scores ≤15, LDLT was associated with superior patient survival (HR = 0.92; 95% c.i. 0.76 to 0.96; P = 0.013). No significant differences in patient survival were observed for MELD scores between 16 and 30. Conversely, for patients with MELD scores >30, LDLT was associated with higher mortality (HR 2.57; 95% c.i. 1.35 to 4.62; P = 0.003). Graft survival was comparable between the two groups for MELD ≤15 and for MELD between 21 and 30. However, for MELD between 16 and 20 (HR = 1.15; 95% c.i. 1.00 to 1.33; P = 0.04) and MELD > 30 (HR = 2.85; 95% c.i. 1.65 to 4.91; P = 0.001), graft survival was considerably shorter after LDLT. Regardless of MELD scores, re-transplantation rate within the first year was significantly higher after LDLT.</p><p><strong>Conclusions: </strong>In this large propensity score-matched study using national data, comparable patient survival was found between LDLT and DDLT in recipients with MELD scores between 16 and 30. Conversely, for patients with MELD > 30, LDLT was associated with worse outcomes. These findings underscore the importance of transplant selection for patients with high MELD scores.</p>","PeriodicalId":9028,"journal":{"name":"BJS Open","volume":"8 3","pages":""},"PeriodicalIF":4.5000,"publicationDate":"2024-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11152206/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJS Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjsopen/zrae058","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: For individuals with advanced liver disease, equipoise in outcomes between live donor liver transplant (LDLT) and deceased donor liver transplant (DDLT) is uncertain.
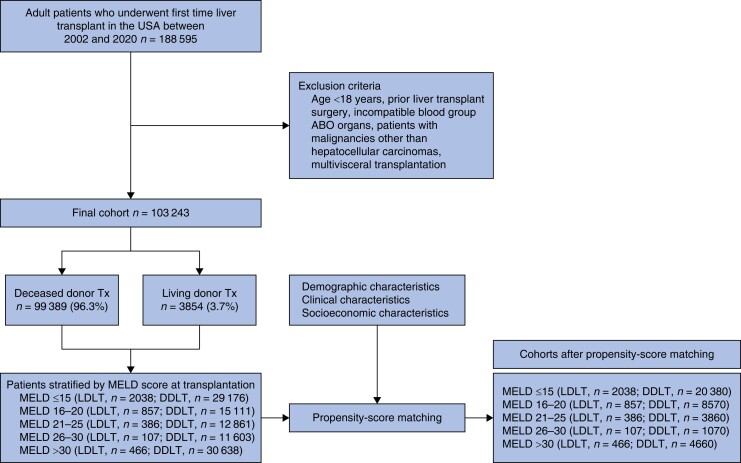
Methods: A retrospective cohort study was performed using data extracted from the Scientific Registry of Transplant Recipients. Adults who underwent first-time DDLT or LTDL in the United States between 2002 and 2020 were paired using propensity-score matching with 1:10 ratio without replacement. Patient and graft survival were compared using the model for end-stage liver disease (MELD) score for stratification.
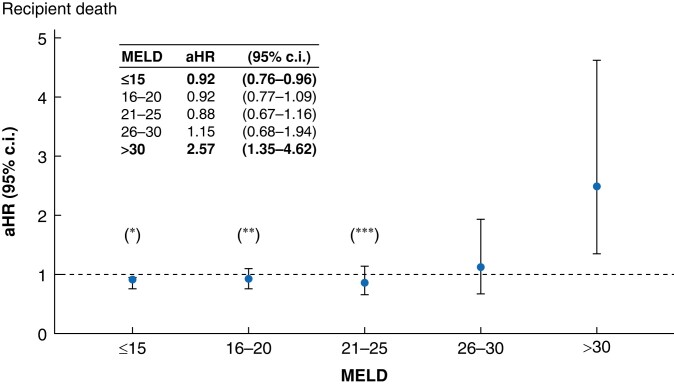
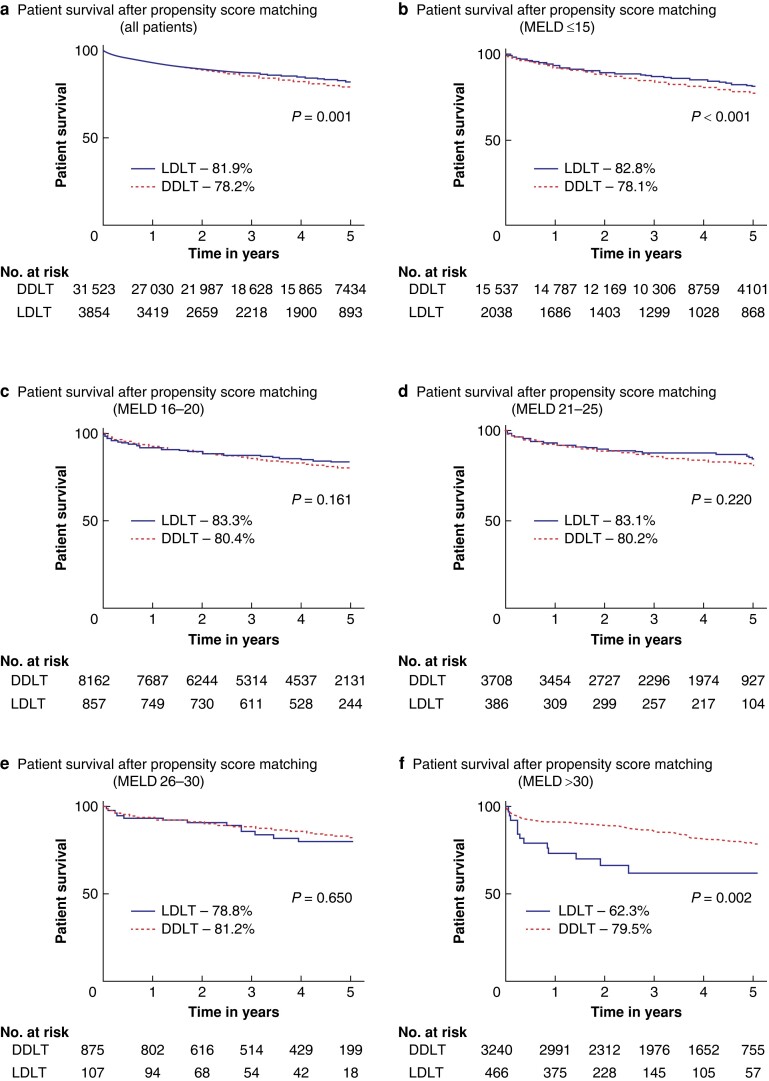
Results: After propensity-score matching, 31 522 DDLT and 3854 LDLT recipients were included. For recipients with MELD scores ≤15, LDLT was associated with superior patient survival (HR = 0.92; 95% c.i. 0.76 to 0.96; P = 0.013). No significant differences in patient survival were observed for MELD scores between 16 and 30. Conversely, for patients with MELD scores >30, LDLT was associated with higher mortality (HR 2.57; 95% c.i. 1.35 to 4.62; P = 0.003). Graft survival was comparable between the two groups for MELD ≤15 and for MELD between 21 and 30. However, for MELD between 16 and 20 (HR = 1.15; 95% c.i. 1.00 to 1.33; P = 0.04) and MELD > 30 (HR = 2.85; 95% c.i. 1.65 to 4.91; P = 0.001), graft survival was considerably shorter after LDLT. Regardless of MELD scores, re-transplantation rate within the first year was significantly higher after LDLT.
Conclusions: In this large propensity score-matched study using national data, comparable patient survival was found between LDLT and DDLT in recipients with MELD scores between 16 and 30. Conversely, for patients with MELD > 30, LDLT was associated with worse outcomes. These findings underscore the importance of transplant selection for patients with high MELD scores.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
