Panagiotis Papamichalis, Katerina G Oikonomou, Maria Xanthoudaki, Asimina Valsamaki, Apostolia-Lemonia Skoura, Sophia K Papathanasiou, Achilleas Chovas
{"title":"Extracorporeal organ support for critically ill patients: Overcoming the past, achieving the maximum at present, and redefining the future.","authors":"Panagiotis Papamichalis, Katerina G Oikonomou, Maria Xanthoudaki, Asimina Valsamaki, Apostolia-Lemonia Skoura, Sophia K Papathanasiou, Achilleas Chovas","doi":"10.5492/wjccm.v13.i2.92458","DOIUrl":null,"url":null,"abstract":"<p><p>Extracorporeal organ support (ECOS) has made remarkable progress over the last few years. Renal replacement therapy, introduced a few decades ago, was the first available application of ECOS. The subsequent evolution of ECOS enabled the enhanced support to many other organs, including the heart [veno-arterial extracorporeal membrane oxygenation (ECMO), slow continuous ultrafiltration], the lungs (veno-venous ECMO, extracorporeal carbon dioxide removal), and the liver (blood purification techniques for the detoxification of liver toxins). Moreover, additional indications of these methods, including the suppression of excessive inflammatory response occurring in severe disorders such as sepsis, coronavirus disease 2019, pancreatitis, and trauma (blood purification techniques for the removal of exotoxins, endotoxins, or cytokines), have arisen. Multiple organ support therapy is crucial since a vast majority of critically ill patients present not with a single but with multiple organ failure (MOF), whereas, traditional therapeutic approaches (mechanical ventilation for acute respiratory failure, antibiotics for sepsis, and inotropes for cardiac dysfunction) have reached the maximum efficacy and cannot be improved further. However, several issues remain to be clarified, such as the complexity and cost of ECOS systems, standardization of indications, therapeutic protocols and initiation time, choice of the patients who will benefit most from these interventions, while evidence from randomized controlled trials supporting their use is still limited. Nevertheless, these methods are currently a part of routine clinical practice in intensive care units. This editorial presents the past, present, and future considerations, as well as perspectives regarding these therapies. Our better understanding of these methods, the pathophysiology of MOF, the crosstalk between native organs resulting in MOF, and the crosstalk between native organs and artificial organ support systems when applied sequentially or simultaneously, will lead to the multiplication of their effects and the minimization of complications arising from their use.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"13 2","pages":"92458"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11155504/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5492/wjccm.v13.i2.92458","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
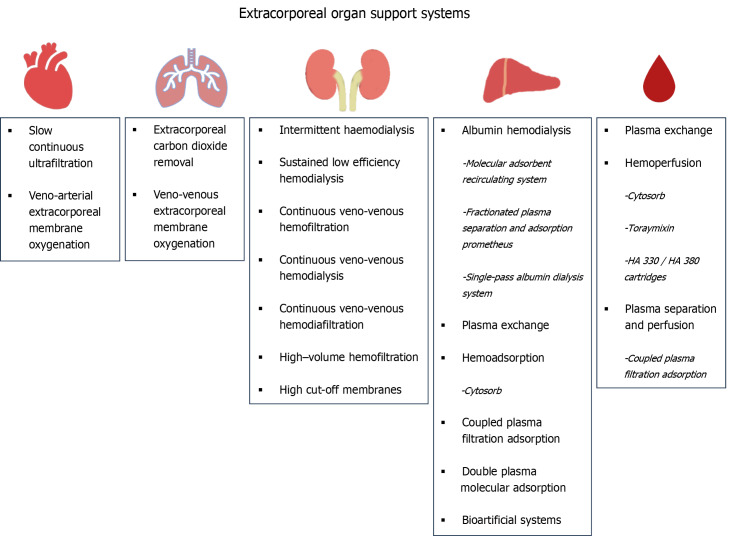
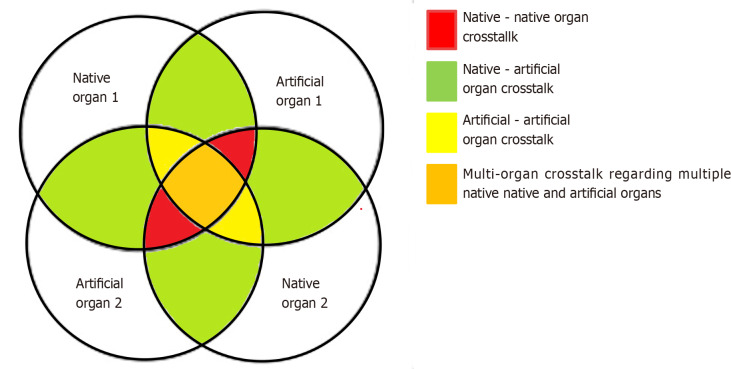
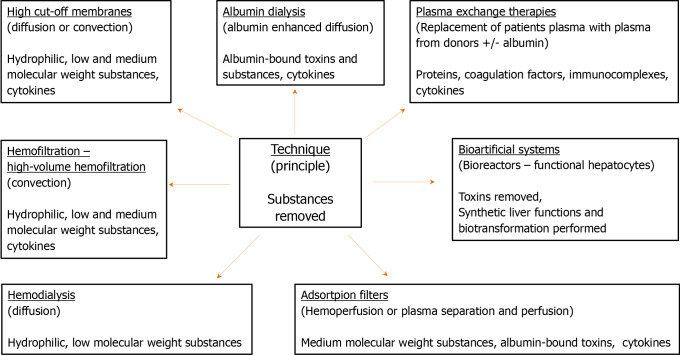
Extracorporeal organ support (ECOS) has made remarkable progress over the last few years. Renal replacement therapy, introduced a few decades ago, was the first available application of ECOS. The subsequent evolution of ECOS enabled the enhanced support to many other organs, including the heart [veno-arterial extracorporeal membrane oxygenation (ECMO), slow continuous ultrafiltration], the lungs (veno-venous ECMO, extracorporeal carbon dioxide removal), and the liver (blood purification techniques for the detoxification of liver toxins). Moreover, additional indications of these methods, including the suppression of excessive inflammatory response occurring in severe disorders such as sepsis, coronavirus disease 2019, pancreatitis, and trauma (blood purification techniques for the removal of exotoxins, endotoxins, or cytokines), have arisen. Multiple organ support therapy is crucial since a vast majority of critically ill patients present not with a single but with multiple organ failure (MOF), whereas, traditional therapeutic approaches (mechanical ventilation for acute respiratory failure, antibiotics for sepsis, and inotropes for cardiac dysfunction) have reached the maximum efficacy and cannot be improved further. However, several issues remain to be clarified, such as the complexity and cost of ECOS systems, standardization of indications, therapeutic protocols and initiation time, choice of the patients who will benefit most from these interventions, while evidence from randomized controlled trials supporting their use is still limited. Nevertheless, these methods are currently a part of routine clinical practice in intensive care units. This editorial presents the past, present, and future considerations, as well as perspectives regarding these therapies. Our better understanding of these methods, the pathophysiology of MOF, the crosstalk between native organs resulting in MOF, and the crosstalk between native organs and artificial organ support systems when applied sequentially or simultaneously, will lead to the multiplication of their effects and the minimization of complications arising from their use.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
