{"title":"Inhaled Corticosteroids Versus Placebo for Stable Chronic Obstructive Pulmonary Disease","authors":"Erin Kamalanathan, Sargam Sharma","doi":"10.1111/cea.14521","DOIUrl":null,"url":null,"abstract":"<p>Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide [<span>1</span>]. It is a chronic noncurable condition, which is defined by progressive respiratory symptoms and airflow limitation. Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2024's guidelines suggest a short-acting beta 2 agonist (SABA) or a long-acting beta 2 agonists (LABA) initially with the addition of a long-acting muscarinic antagonist as necessary. Inhaled corticosteroids (ICS) are considered if a patient falls into Group E. The criteria for Group E include if patients have ≥2 moderate exacerbations or ≥1 leading to hospitalisation and if their eosinophils ≥300 cells per microliter. If a patient has concomitant asthma, patients should be treated following the asthma treatment guideline, so the use of an ICS is mandatory [<span>2</span>].</p><p>Disclaimer: This is an abstract of a Cochrane review ‘Inhaled corticosteroids versus placebo for stable chronic obstructive pulmonary disease’ published in <i>Cochrane Database of Systematic Reviews</i> 2023 Issue 3 10.1002/14651858.cd002991.pub4. Accessed 9 May 2024 (see www.cochranelibrary.com for information). Cochrane reviews are regularly updated as new evidence emerges and in response to feedback, and the Cochrane Library should be consulted for the more recent version of the review.</p><p>Thirty-six primary studies with 23,139 participants met the inclusion criteria. Mean age ranged from 52 to 67 years, and females were 0%–46% of participants. Studies recruited across the severities of COPD. Seventeen studies were of duration longer than 3 months and up to 6 months and 19 studies were of duration longer than 6 months. We judged the overall risk of bias as low.</p><p>Long-term (more than 6 months) use of ICS as monotherapy reduced the mean rate of exacerbations in those studies where pooling of data was possible (generic inverse variance analysis: rate ratio 0.88 exacerbations per participant per year, 95% confidence interval (CI) 0.82–0.94; <i>I</i><sup>2</sup> = 48%, 5 studies, 10,097 participants; moderate-certainty evidence; pooled means analysis: mean difference (MD) −0.05 exacerbations per participant per year, 95% CI −0.07 to −0.02; <i>I</i><sup>2</sup> = 78%, 5 studies, 10,316 participants; moderate-certainty evidence). ICS slowed the rate of decline in quality of life, as measured by the St George's Respiratory Questionnaire (MD −1.22 units/year, 95% CI −1.83 to −0.60; <i>I</i><sup>2</sup> = 0%; 5 studies, 2507 participants; moderate-certainty evidence; minimal clinically importance difference 4 points). There was no evidence of a difference in all-cause mortality in people with COPD (odds ratio (OR) 0.94, 95% CI 0.84–1.07; <i>I</i><sup>2</sup> = 0%; 10 studies, 16,636 participants; moderate-certainty evidence). Long-term use of ICS reduced the rate of decline in FEV1 in people with COPD (generic inverse variance analysis: MD 6.31 mL/year benefit, 95% CI 1.76–10.85; <i>I</i><sup>2</sup> = 0%; 6 studies, 9829 participants; moderate-certainty evidence; pooled means analysis: 7.28 mL/year, 95% CI 3.21–11.35; <i>I</i><sup>2</sup> = 0%; 6 studies, 12,502 participants; moderate-certainty evidence).</p><p>Adverse events: In the long-term studies, the rate of pneumonia was increased in the ICS group, compared with placebo, in studies that reported pneumonia as an adverse event (OR 1.38, 95% CI 1.02–1.88; <i>I</i><sup>2</sup> = 55%; 9 studies, 14,831 participants; low-certainty evidence). There was an increased risk of oropharyngeal candidiasis (OR 2.66, 95% CI 1.91–3.68; 5547 participants) and hoarseness (OR 1.98, 95% CI 1.44–2.74; 3523 participants). The long-term studies that measured bone effects generally showed no major effect on fractures or bone mineral density over 3 years. We downgraded the certainty of evidence to moderate for imprecision and low for imprecision and inconsistency.</p><p>This systematic review included 36 placebo-controlled trials, involving 23,139 participants and aimed to evaluate the benefits and harms of using ICS as monotherapy when compared to placebo in people with stable COPD. Limitations of this systematic review include the heterogeneity of ICS treatment used in the studies, assumed compliance and the inclusion of only stable COPD individuals. Therefore, applying these results to a wider COPD population is difficult. Furthermore, current GOLD guidelines do not suggest ICS as monotherapy but only in addition to dual therapy (LABA and LAMA) if patients have ≥2 moderate exacerbations of COPD per year, history of hospitalisation for exacerbations, blood eosinophils ≥300 cells/μL or history of concomitant asthma. However, the study and evaluation of ICS alone are still clinically relevant due to its widespread use (alongside LABA and LAMA) in COPD, which effects around 174 million people globally [<span>3</span>]. Figure 1 shows meta-analysis of exacerbation rate (mean difference) in ICS versus placebo [<span>4</span>].</p><p>A recent Cochrane review evaluated the use of ICS as dual therapy in a combined SABA/ICS/single inhaler for mild asthma. It showed that the combined use over FABA alone reduced exacerbations, hospital admissions and probably reduces adverse events. Additionally, that FABA/ICS as required was as effective as regular ICS use in reducing asthma-related hospital admissions and less likely to be associated with an increase in adverse events [<span>5</span>]. This supports the conclusion that the potential benefits of introducing regular ICS need to be weighed against adverse events.</p><p>The cost-effectiveness of ICS therapy was not evaluated in this review; currently, the NHS spends roughly 3 billion pounds per year treating COPD [<span>6</span>]. A 2020 study conducted by <i>British Medical Journal</i> (BMJ) aimed to analyse the difference in cost and clinical outcomes between treating a COPD patient according to GOLD or National Institute for Health and Care Excellence (NICE) guidelines compared with current clinical practice. It showed that adhering to GOLD 2020 strategy whereby only introducing triple therapy (LABA, LAMA and ICS) for patients in ‘group D’ (≥2 moderate exacerbations of COPD per year, history of hospitalisation for exacerbations, blood eosinophils ≥300 cells/μL or severe symptoms) resulted in an annual overall reduction in just over £43.7 million, where majority of this cost reduction was associated with pneumonia [<span>7</span>]. This was primarily due to withdrawing ICS in patients who did not meet ‘group D’ criteria and stepping them down to dual therapy. Although the BMJ study used 2020 GOLD guidelines, the new 2024 GOLD Group E criteria are almost identical to the former Group D's criteria; therefore, this cost-effective data still remain clinically relevant.</p><p>This Cochrane review supports the need of further research on clinical and biological factors that predict response to ICS, so that treatment can be specific to individuals and risk of adverse events of ICS potentially reduced.</p><p>E.K. and S.S. contributed equally to this manuscript.</p><p>The author declares no conflicts of interest.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 7","pages":"455-458"},"PeriodicalIF":5.2000,"publicationDate":"2024-06-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14521","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14521","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide [1]. It is a chronic noncurable condition, which is defined by progressive respiratory symptoms and airflow limitation. Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2024's guidelines suggest a short-acting beta 2 agonist (SABA) or a long-acting beta 2 agonists (LABA) initially with the addition of a long-acting muscarinic antagonist as necessary. Inhaled corticosteroids (ICS) are considered if a patient falls into Group E. The criteria for Group E include if patients have ≥2 moderate exacerbations or ≥1 leading to hospitalisation and if their eosinophils ≥300 cells per microliter. If a patient has concomitant asthma, patients should be treated following the asthma treatment guideline, so the use of an ICS is mandatory [2].
Disclaimer: This is an abstract of a Cochrane review ‘Inhaled corticosteroids versus placebo for stable chronic obstructive pulmonary disease’ published in Cochrane Database of Systematic Reviews 2023 Issue 3 10.1002/14651858.cd002991.pub4. Accessed 9 May 2024 (see www.cochranelibrary.com for information). Cochrane reviews are regularly updated as new evidence emerges and in response to feedback, and the Cochrane Library should be consulted for the more recent version of the review.
Thirty-six primary studies with 23,139 participants met the inclusion criteria. Mean age ranged from 52 to 67 years, and females were 0%–46% of participants. Studies recruited across the severities of COPD. Seventeen studies were of duration longer than 3 months and up to 6 months and 19 studies were of duration longer than 6 months. We judged the overall risk of bias as low.
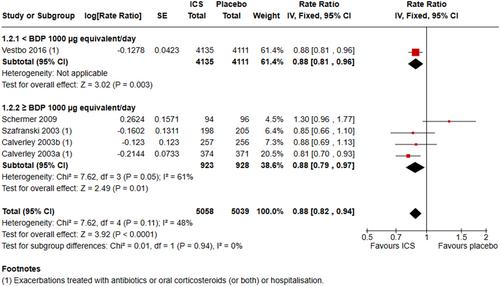
Long-term (more than 6 months) use of ICS as monotherapy reduced the mean rate of exacerbations in those studies where pooling of data was possible (generic inverse variance analysis: rate ratio 0.88 exacerbations per participant per year, 95% confidence interval (CI) 0.82–0.94; I2 = 48%, 5 studies, 10,097 participants; moderate-certainty evidence; pooled means analysis: mean difference (MD) −0.05 exacerbations per participant per year, 95% CI −0.07 to −0.02; I2 = 78%, 5 studies, 10,316 participants; moderate-certainty evidence). ICS slowed the rate of decline in quality of life, as measured by the St George's Respiratory Questionnaire (MD −1.22 units/year, 95% CI −1.83 to −0.60; I2 = 0%; 5 studies, 2507 participants; moderate-certainty evidence; minimal clinically importance difference 4 points). There was no evidence of a difference in all-cause mortality in people with COPD (odds ratio (OR) 0.94, 95% CI 0.84–1.07; I2 = 0%; 10 studies, 16,636 participants; moderate-certainty evidence). Long-term use of ICS reduced the rate of decline in FEV1 in people with COPD (generic inverse variance analysis: MD 6.31 mL/year benefit, 95% CI 1.76–10.85; I2 = 0%; 6 studies, 9829 participants; moderate-certainty evidence; pooled means analysis: 7.28 mL/year, 95% CI 3.21–11.35; I2 = 0%; 6 studies, 12,502 participants; moderate-certainty evidence).
Adverse events: In the long-term studies, the rate of pneumonia was increased in the ICS group, compared with placebo, in studies that reported pneumonia as an adverse event (OR 1.38, 95% CI 1.02–1.88; I2 = 55%; 9 studies, 14,831 participants; low-certainty evidence). There was an increased risk of oropharyngeal candidiasis (OR 2.66, 95% CI 1.91–3.68; 5547 participants) and hoarseness (OR 1.98, 95% CI 1.44–2.74; 3523 participants). The long-term studies that measured bone effects generally showed no major effect on fractures or bone mineral density over 3 years. We downgraded the certainty of evidence to moderate for imprecision and low for imprecision and inconsistency.
This systematic review included 36 placebo-controlled trials, involving 23,139 participants and aimed to evaluate the benefits and harms of using ICS as monotherapy when compared to placebo in people with stable COPD. Limitations of this systematic review include the heterogeneity of ICS treatment used in the studies, assumed compliance and the inclusion of only stable COPD individuals. Therefore, applying these results to a wider COPD population is difficult. Furthermore, current GOLD guidelines do not suggest ICS as monotherapy but only in addition to dual therapy (LABA and LAMA) if patients have ≥2 moderate exacerbations of COPD per year, history of hospitalisation for exacerbations, blood eosinophils ≥300 cells/μL or history of concomitant asthma. However, the study and evaluation of ICS alone are still clinically relevant due to its widespread use (alongside LABA and LAMA) in COPD, which effects around 174 million people globally [3]. Figure 1 shows meta-analysis of exacerbation rate (mean difference) in ICS versus placebo [4].
A recent Cochrane review evaluated the use of ICS as dual therapy in a combined SABA/ICS/single inhaler for mild asthma. It showed that the combined use over FABA alone reduced exacerbations, hospital admissions and probably reduces adverse events. Additionally, that FABA/ICS as required was as effective as regular ICS use in reducing asthma-related hospital admissions and less likely to be associated with an increase in adverse events [5]. This supports the conclusion that the potential benefits of introducing regular ICS need to be weighed against adverse events.
The cost-effectiveness of ICS therapy was not evaluated in this review; currently, the NHS spends roughly 3 billion pounds per year treating COPD [6]. A 2020 study conducted by British Medical Journal (BMJ) aimed to analyse the difference in cost and clinical outcomes between treating a COPD patient according to GOLD or National Institute for Health and Care Excellence (NICE) guidelines compared with current clinical practice. It showed that adhering to GOLD 2020 strategy whereby only introducing triple therapy (LABA, LAMA and ICS) for patients in ‘group D’ (≥2 moderate exacerbations of COPD per year, history of hospitalisation for exacerbations, blood eosinophils ≥300 cells/μL or severe symptoms) resulted in an annual overall reduction in just over £43.7 million, where majority of this cost reduction was associated with pneumonia [7]. This was primarily due to withdrawing ICS in patients who did not meet ‘group D’ criteria and stepping them down to dual therapy. Although the BMJ study used 2020 GOLD guidelines, the new 2024 GOLD Group E criteria are almost identical to the former Group D's criteria; therefore, this cost-effective data still remain clinically relevant.
This Cochrane review supports the need of further research on clinical and biological factors that predict response to ICS, so that treatment can be specific to individuals and risk of adverse events of ICS potentially reduced.
E.K. and S.S. contributed equally to this manuscript.
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
