{"title":"Noradrenaline infusion prevents anesthesia-induced hypotension in severe aortic stenosis patients undergoing transcatheter aortic valve replacement: a retrospective observational study.","authors":"Kenta Onishi, Masashi Yoshida, Hisakatsu Ito, Masaaki Kawakami, Tomonori Takazawa","doi":"10.1186/s40981-024-00721-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with severe aortic valve stenosis (AS) are particularly prone to developing hypotension during general anesthesia induction, which increases postoperative morbidity and mortality. Although the preventive effect of a single vasopressor dose on anesthesia-induced hypotension has been reported, the effects of continuous vasopressor infusion are unknown. This study aimed to assess the effect of noradrenaline (NAd) infusion on hemodynamic stability during general anesthesia induction in severe AS patients undergoing transcatheter aortic valve replacement (TAVR).</p><p><strong>Methods: </strong>This single-center, retrospective study included severe AS patients who underwent elective TAVR. Patients in the NAd group received a continuous prophylactic NAd infusion of 0.1 μg/kg/min from the time of anesthesia induction. The control group received inotropes and vasopressors as indicated by the occurrence of hypotension. The primary outcome was the lowest mean blood pressure (MBP) before the start of surgery.</p><p><strong>Results: </strong>The study included 68 patients in the NAd group and 113 in the control group. The lowest MBP before the start of surgery was significantly higher in the NAd group than in the control group (63 ± 15 vs 47 ± 13 mmHg, P < 0.01). MBP immediately before intubation was also significantly higher in the NAd group (75 ± 17 vs 57 ± 16 mmHg, P < 0.01). Differences in postoperative complications between the groups were negligible.</p><p><strong>Conclusion: </strong>Continuous administration of NAd at 0.1 μg/kg/min in patients with severe AS might prevent hypotension during general anesthesia induction for TAVR.</p>","PeriodicalId":14635,"journal":{"name":"JA Clinical Reports","volume":"10 1","pages":"39"},"PeriodicalIF":1.0000,"publicationDate":"2024-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11176125/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JA Clinical Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40981-024-00721-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with severe aortic valve stenosis (AS) are particularly prone to developing hypotension during general anesthesia induction, which increases postoperative morbidity and mortality. Although the preventive effect of a single vasopressor dose on anesthesia-induced hypotension has been reported, the effects of continuous vasopressor infusion are unknown. This study aimed to assess the effect of noradrenaline (NAd) infusion on hemodynamic stability during general anesthesia induction in severe AS patients undergoing transcatheter aortic valve replacement (TAVR).
Methods: This single-center, retrospective study included severe AS patients who underwent elective TAVR. Patients in the NAd group received a continuous prophylactic NAd infusion of 0.1 μg/kg/min from the time of anesthesia induction. The control group received inotropes and vasopressors as indicated by the occurrence of hypotension. The primary outcome was the lowest mean blood pressure (MBP) before the start of surgery.
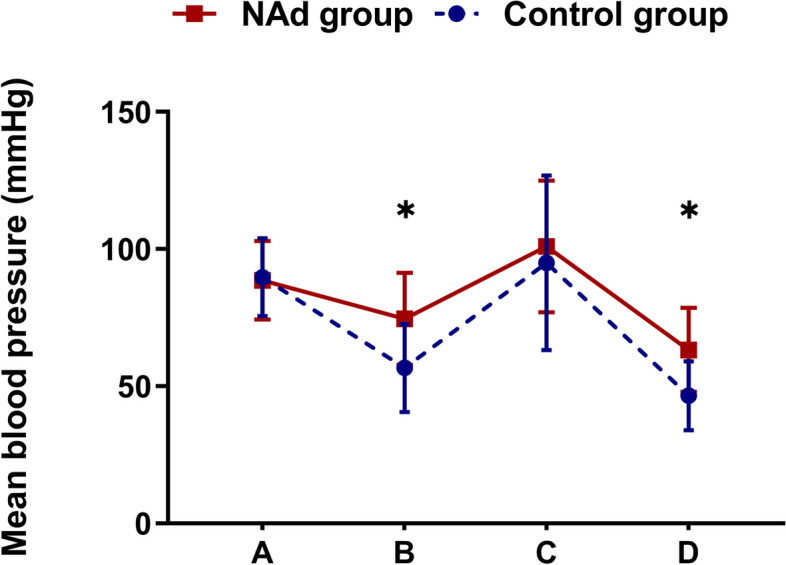
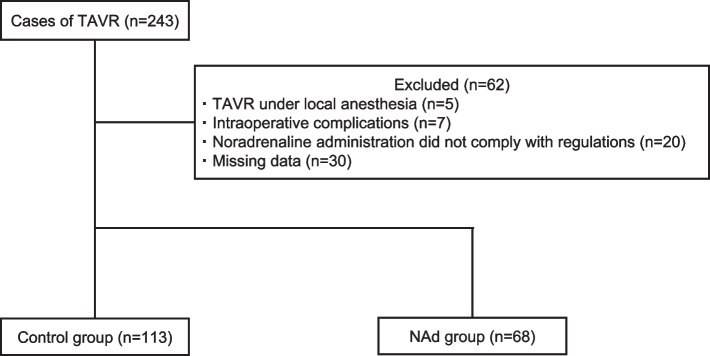
Results: The study included 68 patients in the NAd group and 113 in the control group. The lowest MBP before the start of surgery was significantly higher in the NAd group than in the control group (63 ± 15 vs 47 ± 13 mmHg, P < 0.01). MBP immediately before intubation was also significantly higher in the NAd group (75 ± 17 vs 57 ± 16 mmHg, P < 0.01). Differences in postoperative complications between the groups were negligible.
Conclusion: Continuous administration of NAd at 0.1 μg/kg/min in patients with severe AS might prevent hypotension during general anesthesia induction for TAVR.
期刊介绍:
JA Clinical Reports is a companion journal to the Journal of Anesthesia (JA), the official journal of the Japanese Society of Anesthesiologists (JSA). This journal is an open access, peer-reviewed, online journal related to clinical anesthesia practices such as anesthesia management, pain management and intensive care. Case reports are very important articles from the viewpoint of education and the cultivation of scientific thinking in the field of anesthesia. However, submissions of anesthesia research and clinical reports from Japan are notably decreasing in major anesthesia journals. Therefore, the JSA has decided to launch a new journal, JA Clinical Reports, to encourage JSA members, particularly junior Japanese anesthesiologists, to publish papers in English language.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
