{"title":"Hypotension prediction index for prevention of intraoperative hypotension in patients undergoing general anesthesia: a randomized controlled trial.","authors":"Chih-Jun Lai, Ya-Jung Cheng, Yin-Yi Han, Po-Ni Hsiao, Pei-Lin Lin, Ching-Tang Chiu, Jang-Ming Lee, Yu-Wen Tien, Kuo-Liong Chien","doi":"10.1186/s13741-024-00414-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intraoperative hypotension is a common side effect of general anesthesia. Here we examined whether the Hypotension Prediction Index (HPI), a novel warning system, reduces the severity and duration of intraoperative hypotension during general anesthesia.</p><p><strong>Methods: </strong>This randomized controlled trial was conducted in a tertiary referral hospital. We enrolled patients undergoing general anesthesia with invasive arterial monitoring. Patients were randomized 1:1 either to receive hemodynamic management with HPI guidance (intervention) or standard of care (control) treatment. Intraoperative hypotension treatment was initiated at HPI > 85 (intervention) or mean arterial pressure (MAP) < 65 mmHg (control). The primary outcome was hypotension severity, defined as a time-weighted average (TWA) MAP < 65 mmHg. Secondary outcomes were TWA MAP < 60 and < 55 mmHg.</p><p><strong>Results: </strong>Of the 60 patients who completed the study, 30 were in the intervention group and 30 in the control group. The patients' median age was 62 years, and 48 of them were male. The median duration of surgery was 490 min. The median MAP before surgery presented no significant difference between the two groups. The intervention group showed significantly lower median TWA MAP < 65 mmHg than the control group (0.02 [0.003, 0.08] vs. 0.37 [0.20, 0.58], P < 0.001). Findings were similar for TWA MAP < 60 mmHg and < 55 mmHg. The median MAP during surgery was significantly higher in the intervention group than that in the control group (87.54 mmHg vs. 77.92 mmHg, P < 0.001).</p><p><strong>Conclusions: </strong>HPI guidance appears to be effective in preventing intraoperative hypotension during general anesthesia. Further investigation is needed to assess the impact of HPI on patient outcomes.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov (NCT04966364); 202105065RINA; Date of registration: July 19, 2021; The recruitment date of the first patient: July 22, 2021.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"13 1","pages":"57"},"PeriodicalIF":2.1000,"publicationDate":"2024-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11180403/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-024-00414-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Intraoperative hypotension is a common side effect of general anesthesia. Here we examined whether the Hypotension Prediction Index (HPI), a novel warning system, reduces the severity and duration of intraoperative hypotension during general anesthesia.
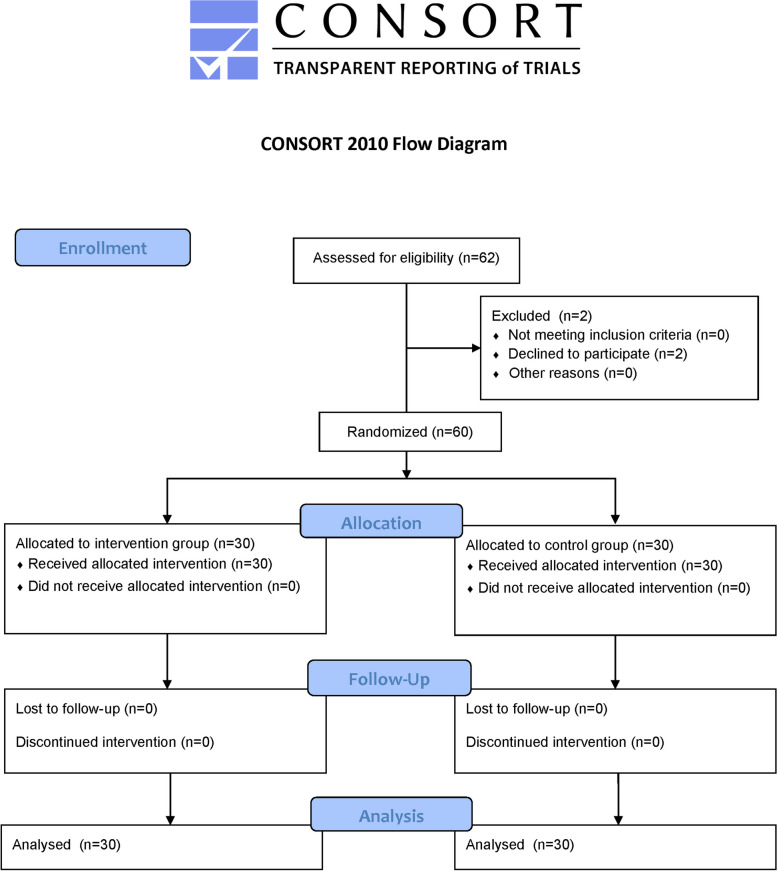
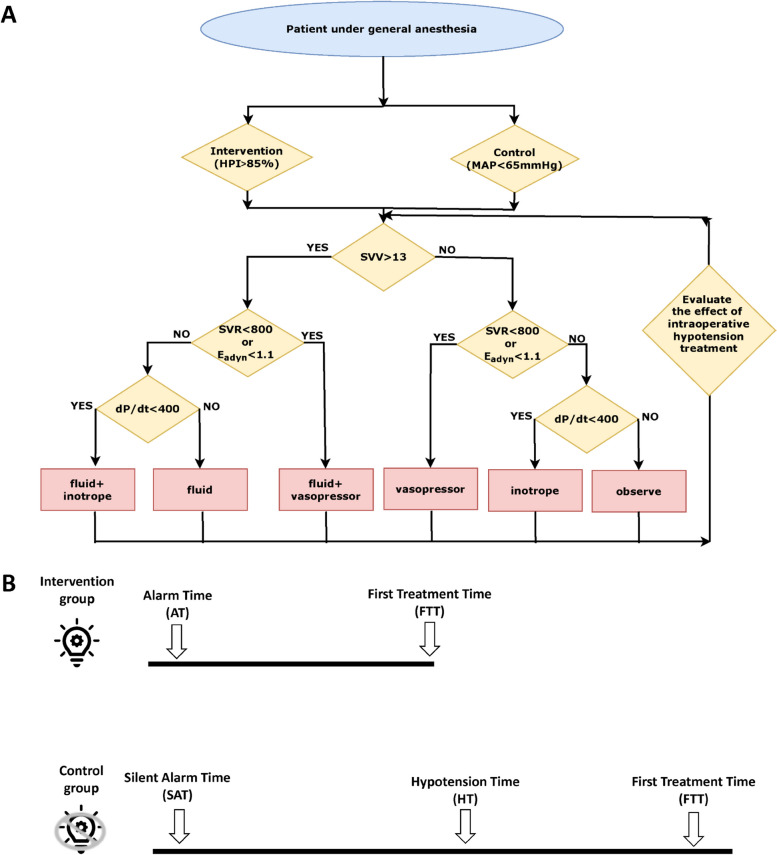
Methods: This randomized controlled trial was conducted in a tertiary referral hospital. We enrolled patients undergoing general anesthesia with invasive arterial monitoring. Patients were randomized 1:1 either to receive hemodynamic management with HPI guidance (intervention) or standard of care (control) treatment. Intraoperative hypotension treatment was initiated at HPI > 85 (intervention) or mean arterial pressure (MAP) < 65 mmHg (control). The primary outcome was hypotension severity, defined as a time-weighted average (TWA) MAP < 65 mmHg. Secondary outcomes were TWA MAP < 60 and < 55 mmHg.
Results: Of the 60 patients who completed the study, 30 were in the intervention group and 30 in the control group. The patients' median age was 62 years, and 48 of them were male. The median duration of surgery was 490 min. The median MAP before surgery presented no significant difference between the two groups. The intervention group showed significantly lower median TWA MAP < 65 mmHg than the control group (0.02 [0.003, 0.08] vs. 0.37 [0.20, 0.58], P < 0.001). Findings were similar for TWA MAP < 60 mmHg and < 55 mmHg. The median MAP during surgery was significantly higher in the intervention group than that in the control group (87.54 mmHg vs. 77.92 mmHg, P < 0.001).
Conclusions: HPI guidance appears to be effective in preventing intraoperative hypotension during general anesthesia. Further investigation is needed to assess the impact of HPI on patient outcomes.
Trial registration: ClinicalTrials.gov (NCT04966364); 202105065RINA; Date of registration: July 19, 2021; The recruitment date of the first patient: July 22, 2021.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
