{"title":"Association Between Health Insurance Status and Quality of Life Among People With Asthma in Kolkata","authors":"Sudipta Nandan, Prasun Haldar, Paige Lacy, Saibal Moitra, Subhabrata Moitra","doi":"10.1111/cea.14524","DOIUrl":null,"url":null,"abstract":"<p>Out-of-pocket expenditure for chronic diseases poses a significant economic burden, especially in low- and middle-income countries such as India [<span>1</span>]. Asthma, affecting one in every 50 people in India, accounts for nearly one-tenth of the global asthma population [<span>2</span>]. According to an estimate, the annual cost of asthma treatment per patient is about $240, totalling approximately $9.41 billion annually in India [<span>3</span>]. Despite numerous health schemes of provincial or federal governments, availability of health insurance from the government or privately owned insurance companies and complementary health insurance for employees in most sectors, nearly 60% of all Indians do not possess any health insurance policies. Moreover, most health insurance schemes do not cover physician consultation at an outpatient clinic. Although the disparity in healthcare coverage is recognised as a factor in the economic burden of asthma, there is a lack of studies on the specific role of health insurance on the health-related quality of life (HRQL) in asthma patients.</p><p>In this cross-sectional study, we recruited 224 mild-to-moderate adult asthma patients from two tertiary healthcare facilities in Kolkata. We collected demographic information, such as age, sex, body mass index (BMI), education, employment, addiction (smoking and alcohol consumption), family type (nuclear/joint) and health insurance (yes/no) by questionnaire. Asthma was physician-diagnosed. Comorbidity was assessed by the Charlson Comorbidity Index (CCI) [<span>4</span>]. Asthma control was assessed by the asthma control test (ACT) and was categorised as well-controlled (score ≥ 20), partially controlled (score 16–19) and poorly controlled (score < 16) as per the established guidelines [<span>5</span>]. HRQL was assessed using the asthma quality-of-life questionnaire (AQLQ) [<span>6</span>]. All questionnaires were self-administered, utilising prevalidated Bengali versions of the ACT and AQLQ. The study was approved by the Human Research Ethics Committee of the Allergy & Asthma Research Centre, Kolkata (CREC-AARC-0027/18), and participants provided signed informed consent. The repository shows the demographic and clinical characteristics of the study participants.</p><p>Descriptive statistics were presented as mean (standard deviation [SD]), median (interquartile range [IQR]) or frequencies (%) as appropriate. We constructed multivariable linear regression models to test the associations between health insurance and AQLQ total and subdomain scores adjusted for age, sex, education, employment status, alcohol consumption and CCI score. We stratified the models by sex and asthma control as specified earlier and compared the estimates between sex and asthma control groups using the Wald test.</p><p>Based on the a priori mean (SD) of the AQLQ total score of 5.24 (0.67) in a previously published report [<span>7</span>], our sample size achieved 100% power to detect a clinically important difference in the AQLQ score. 56% of the patients were female (mean age of 35 ± 16 years). 12% were smokers, and 35% reported possessing health insurance. 63% had well-controlled asthma, whereas 15% and 22% reported partially controlled and poorly controlled asthma, respectively. The mean (SD) AQLQ total score was 5.6 (1.1). In linear models adjusted for confounders, possessing health insurance was associated with a better AQLQ total score (regression coefficient [<i>β</i>]: 0.66; 95% confidence interval [CI]: 0.33, 1.00). We observed similar associations between health insurance and AQLQ symptom score (<i>β</i>: 0.60; 95% CI: 0.25, 0.97), activity limitation (<i>β</i>: 0.78; 95% CI: 0.41, 1.14), emotional function (<i>β</i>: 0.60; 95% CI: 0.20, 1.00) and environmental stimuli score (<i>β</i>: 0.64; 95% CI: 0.21, 1.07). Additional materials can be found at https://osf.io/58x3h/.</p><p>We found that the association between health insurance and higher AQLQ total scores was statistically significant for both males and females. However, the association was notably stronger in males (<i>β</i>: 0.88; 95% CI: 0.40, 1.36) than in females (<i>β</i>: 0.48; 95% CI: 0.004, 0.96), with a Wald test <i>p</i>-value < 0.05, indicating a significant difference. Except for the activity limitation subdomain, associations between health insurance and other AQLQ subdomain scores were consistently significant in males but not in females, with significant differences in magnitude between sexes (Figure 1A). When stratified by asthma control, the associations between health insurance and AQLQ total and subdomain scores were significant only in the well-controlled group, and not in the partially or poorly controlled groups (Figure 1B).</p><p>We observed that health insurance is significantly associated with better quality of life in asthma. This association is stronger among males than among females. Also, health insurance is associated with better quality of life only among asthma patients whose symptoms are well-controlled, but the associations were inconsistent in patients with partially or poorly controlled asthma. The rising economic disparity is a major concern in most low- and middle-income countries with an increasing prevalence of noncommunicable diseases [<span>1</span>]. Our findings are relatable to other studies on out-of-pocket expenditure in relation to poor HRQL in patients with diabetes, hypertension and chronic kidney diseases [<span>8, 9</span>]. Therefore, more large-scale epidemiological studies are required for a better understanding of the economic impact of asthma on HRQL.</p><p>Our study is the first report to demonstrate the importance of health insurance in patients with chronic diseases such as asthma including participants of all ages and varying levels of symptom control. However, limitations include a lack of information about socio-economic status, place of residence, healthcare access and annual healthcare costs. Also, we could not capture information about disease severity, current treatment and compliance, which would have provided a more detailed view of the economic burden alongside health insurance coverage. Moreover, we could not determine the role of the limit (capping) of health insurance on out-of-pocket expenses. Our study discusses a pertinent issue of the global burden of asthma and advocates for more inclusive and universal healthcare coverage in India, particularly for the marginalised population. Nevertheless, it must be remembered that proper diagnosis, treatment and awareness of disease symptoms remain crucial determinants of HRQL in asthma.</p><p>Su.M. conceptualised the study, performed the data analysis and wrote the manuscript. S.N. and S.M. collected and interpreted data and revised the manuscript. P.H. curated the data and revised the manuscript. P.L. revised the manuscript. Su.M. takes responsibility for the integrity of the study and the publication of the manuscript.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 9","pages":"709-711"},"PeriodicalIF":5.2000,"publicationDate":"2024-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14524","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14524","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Out-of-pocket expenditure for chronic diseases poses a significant economic burden, especially in low- and middle-income countries such as India [1]. Asthma, affecting one in every 50 people in India, accounts for nearly one-tenth of the global asthma population [2]. According to an estimate, the annual cost of asthma treatment per patient is about $240, totalling approximately $9.41 billion annually in India [3]. Despite numerous health schemes of provincial or federal governments, availability of health insurance from the government or privately owned insurance companies and complementary health insurance for employees in most sectors, nearly 60% of all Indians do not possess any health insurance policies. Moreover, most health insurance schemes do not cover physician consultation at an outpatient clinic. Although the disparity in healthcare coverage is recognised as a factor in the economic burden of asthma, there is a lack of studies on the specific role of health insurance on the health-related quality of life (HRQL) in asthma patients.
In this cross-sectional study, we recruited 224 mild-to-moderate adult asthma patients from two tertiary healthcare facilities in Kolkata. We collected demographic information, such as age, sex, body mass index (BMI), education, employment, addiction (smoking and alcohol consumption), family type (nuclear/joint) and health insurance (yes/no) by questionnaire. Asthma was physician-diagnosed. Comorbidity was assessed by the Charlson Comorbidity Index (CCI) [4]. Asthma control was assessed by the asthma control test (ACT) and was categorised as well-controlled (score ≥ 20), partially controlled (score 16–19) and poorly controlled (score < 16) as per the established guidelines [5]. HRQL was assessed using the asthma quality-of-life questionnaire (AQLQ) [6]. All questionnaires were self-administered, utilising prevalidated Bengali versions of the ACT and AQLQ. The study was approved by the Human Research Ethics Committee of the Allergy & Asthma Research Centre, Kolkata (CREC-AARC-0027/18), and participants provided signed informed consent. The repository shows the demographic and clinical characteristics of the study participants.
Descriptive statistics were presented as mean (standard deviation [SD]), median (interquartile range [IQR]) or frequencies (%) as appropriate. We constructed multivariable linear regression models to test the associations between health insurance and AQLQ total and subdomain scores adjusted for age, sex, education, employment status, alcohol consumption and CCI score. We stratified the models by sex and asthma control as specified earlier and compared the estimates between sex and asthma control groups using the Wald test.
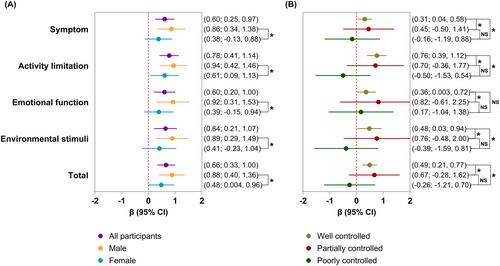
Based on the a priori mean (SD) of the AQLQ total score of 5.24 (0.67) in a previously published report [7], our sample size achieved 100% power to detect a clinically important difference in the AQLQ score. 56% of the patients were female (mean age of 35 ± 16 years). 12% were smokers, and 35% reported possessing health insurance. 63% had well-controlled asthma, whereas 15% and 22% reported partially controlled and poorly controlled asthma, respectively. The mean (SD) AQLQ total score was 5.6 (1.1). In linear models adjusted for confounders, possessing health insurance was associated with a better AQLQ total score (regression coefficient [β]: 0.66; 95% confidence interval [CI]: 0.33, 1.00). We observed similar associations between health insurance and AQLQ symptom score (β: 0.60; 95% CI: 0.25, 0.97), activity limitation (β: 0.78; 95% CI: 0.41, 1.14), emotional function (β: 0.60; 95% CI: 0.20, 1.00) and environmental stimuli score (β: 0.64; 95% CI: 0.21, 1.07). Additional materials can be found at https://osf.io/58x3h/.
We found that the association between health insurance and higher AQLQ total scores was statistically significant for both males and females. However, the association was notably stronger in males (β: 0.88; 95% CI: 0.40, 1.36) than in females (β: 0.48; 95% CI: 0.004, 0.96), with a Wald test p-value < 0.05, indicating a significant difference. Except for the activity limitation subdomain, associations between health insurance and other AQLQ subdomain scores were consistently significant in males but not in females, with significant differences in magnitude between sexes (Figure 1A). When stratified by asthma control, the associations between health insurance and AQLQ total and subdomain scores were significant only in the well-controlled group, and not in the partially or poorly controlled groups (Figure 1B).
We observed that health insurance is significantly associated with better quality of life in asthma. This association is stronger among males than among females. Also, health insurance is associated with better quality of life only among asthma patients whose symptoms are well-controlled, but the associations were inconsistent in patients with partially or poorly controlled asthma. The rising economic disparity is a major concern in most low- and middle-income countries with an increasing prevalence of noncommunicable diseases [1]. Our findings are relatable to other studies on out-of-pocket expenditure in relation to poor HRQL in patients with diabetes, hypertension and chronic kidney diseases [8, 9]. Therefore, more large-scale epidemiological studies are required for a better understanding of the economic impact of asthma on HRQL.
Our study is the first report to demonstrate the importance of health insurance in patients with chronic diseases such as asthma including participants of all ages and varying levels of symptom control. However, limitations include a lack of information about socio-economic status, place of residence, healthcare access and annual healthcare costs. Also, we could not capture information about disease severity, current treatment and compliance, which would have provided a more detailed view of the economic burden alongside health insurance coverage. Moreover, we could not determine the role of the limit (capping) of health insurance on out-of-pocket expenses. Our study discusses a pertinent issue of the global burden of asthma and advocates for more inclusive and universal healthcare coverage in India, particularly for the marginalised population. Nevertheless, it must be remembered that proper diagnosis, treatment and awareness of disease symptoms remain crucial determinants of HRQL in asthma.
Su.M. conceptualised the study, performed the data analysis and wrote the manuscript. S.N. and S.M. collected and interpreted data and revised the manuscript. P.H. curated the data and revised the manuscript. P.L. revised the manuscript. Su.M. takes responsibility for the integrity of the study and the publication of the manuscript.
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
