Christopher Licskai, Anna Hussey, Véronique Rowley, Madonna Ferrone, Zihang Lu, Kimball Zhang, Emilie Terebessy, Andrew Scarffe, Shannon Sibbald, Cathy Faulds, Tim O'Callahan, Teresa To
{"title":"Quantifying sustained health system benefits of primary care-based integrated disease management for COPD: a 6-year interrupted time series study.","authors":"Christopher Licskai, Anna Hussey, Véronique Rowley, Madonna Ferrone, Zihang Lu, Kimball Zhang, Emilie Terebessy, Andrew Scarffe, Shannon Sibbald, Cathy Faulds, Tim O'Callahan, Teresa To","doi":"10.1136/thorax-2023-221211","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Severe exacerbation of chronic obstructive pulmonary disease (COPD) is a trajectory-changing life event for patients and a major contributor to health system costs. This study evaluates the real-world impact of a primary care, integrated disease management (IDM) programme on acute health service utilisation (HSU) in the Canadian health system.</p><p><strong>Methods: </strong>Interrupted time series analysis using retrospective health administrative data, comparing monthly HSU event rates 3 years prior to and 3 years following the implementation of COPD IDM. Primary outcomes were COPD-related hospitalisation and emergency department (ED) visits. Secondary outcomes included hospital bed days and all-cause HSU.</p><p><strong>Results: </strong>There were 2451 participants. COPD-related and all-cause HSU rates increased in the 3 years prior to IDM implementation. With implementation, there was an immediate decrease (month 1) in COPD-related hospitalisation and ED visit rates of -4.6 (95% CI: -7.76 to -1.39) and -6.2 (95% CI: -11.88, -0.48) per 1000 participants per month, respectively, compared with the counterfactual control group. After 12 months, COPD-related hospitalisation rates decreased: -9.1 events per 1000 participants per month (95% CI: -12.72, -5.44) and ED visits -19.0 (95% CI: -25.50, -12.46). This difference nearly doubled by 36 months. All-cause HSU also demonstrated rate reductions at 12 months, hospitalisation was -10.2 events per 1000 participants per month (95% CI: -15.79, -4.44) and ED visits were -30.4 (95% CI: -41.95, -18.78).</p><p><strong>Conclusions: </strong>Implementation of COPD IDM in a primary care setting was associated with a changed trajectory of COPD-related and all-cause HSU from an increasing year-on-year trend to sustained long-term reductions. This highlights a substantial real-world opportunity that may improve health system performance and patient outcomes.</p>","PeriodicalId":23284,"journal":{"name":"Thorax","volume":" ","pages":"725-734"},"PeriodicalIF":7.7000,"publicationDate":"2024-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11287652/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thorax","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/thorax-2023-221211","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Severe exacerbation of chronic obstructive pulmonary disease (COPD) is a trajectory-changing life event for patients and a major contributor to health system costs. This study evaluates the real-world impact of a primary care, integrated disease management (IDM) programme on acute health service utilisation (HSU) in the Canadian health system.
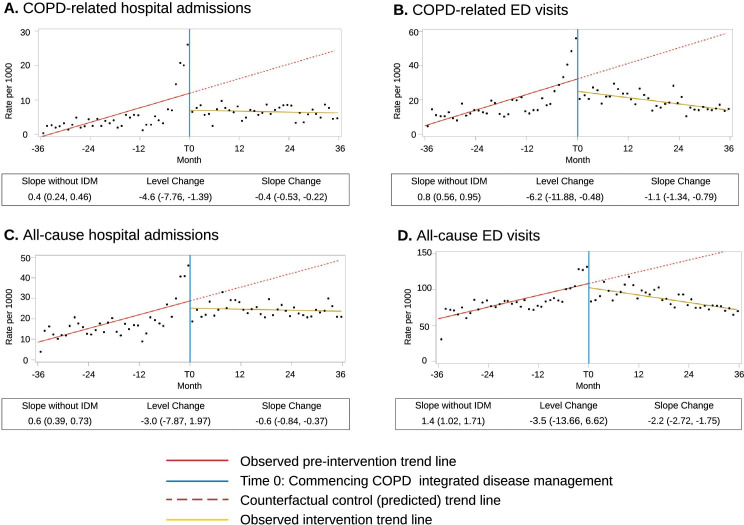
Methods: Interrupted time series analysis using retrospective health administrative data, comparing monthly HSU event rates 3 years prior to and 3 years following the implementation of COPD IDM. Primary outcomes were COPD-related hospitalisation and emergency department (ED) visits. Secondary outcomes included hospital bed days and all-cause HSU.
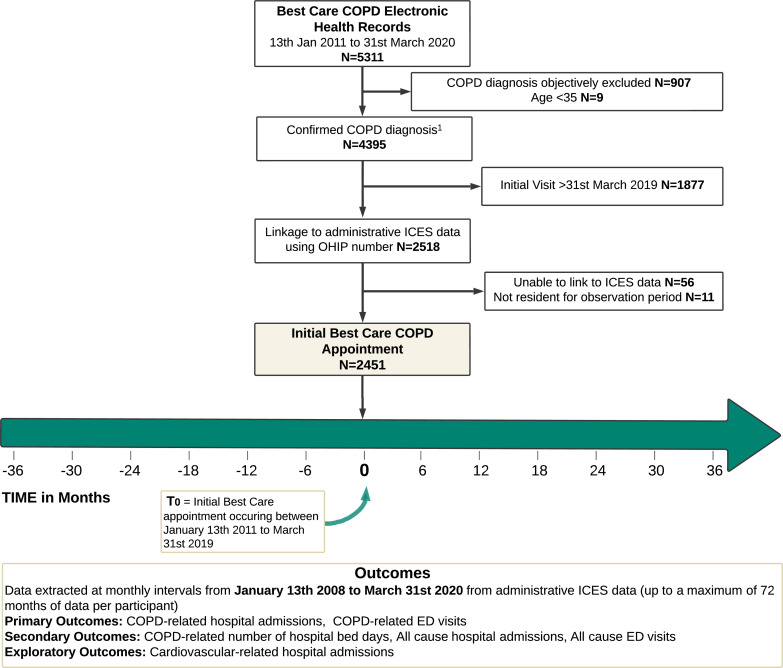
Results: There were 2451 participants. COPD-related and all-cause HSU rates increased in the 3 years prior to IDM implementation. With implementation, there was an immediate decrease (month 1) in COPD-related hospitalisation and ED visit rates of -4.6 (95% CI: -7.76 to -1.39) and -6.2 (95% CI: -11.88, -0.48) per 1000 participants per month, respectively, compared with the counterfactual control group. After 12 months, COPD-related hospitalisation rates decreased: -9.1 events per 1000 participants per month (95% CI: -12.72, -5.44) and ED visits -19.0 (95% CI: -25.50, -12.46). This difference nearly doubled by 36 months. All-cause HSU also demonstrated rate reductions at 12 months, hospitalisation was -10.2 events per 1000 participants per month (95% CI: -15.79, -4.44) and ED visits were -30.4 (95% CI: -41.95, -18.78).
Conclusions: Implementation of COPD IDM in a primary care setting was associated with a changed trajectory of COPD-related and all-cause HSU from an increasing year-on-year trend to sustained long-term reductions. This highlights a substantial real-world opportunity that may improve health system performance and patient outcomes.
期刊介绍:
Thorax stands as one of the premier respiratory medicine journals globally, featuring clinical and experimental research articles spanning respiratory medicine, pediatrics, immunology, pharmacology, pathology, and surgery. The journal's mission is to publish noteworthy advancements in scientific understanding that are poised to influence clinical practice significantly. This encompasses articles delving into basic and translational mechanisms applicable to clinical material, covering areas such as cell and molecular biology, genetics, epidemiology, and immunology.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
