Kimberley J. Davis, Chantal Campbell, Rebekah Costelloe, Ting Song, Glaucia Fylyk, Ping Yu, Steven J. Craig
{"title":"Causes of Unwarranted Variation and Disparity in Breast Cancer Management in Regional and Rural Area","authors":"Kimberley J. Davis, Chantal Campbell, Rebekah Costelloe, Ting Song, Glaucia Fylyk, Ping Yu, Steven J. Craig","doi":"10.1155/2024/9354395","DOIUrl":null,"url":null,"abstract":"<div>\n <p><i>Introduction</i>. Breast cancer management is complex, requiring personalised care from multidisciplinary teams. Research shows that there is unwarranted clinical variation in mastectomy rates between rural and metropolitan patients; that is, variation in treatment which cannot be explained by disease progression or medical necessity. This study aims to determine the clinical and nonclinical factors contributing to any unwarranted variation in breast cancer management in rural patients and to evaluate how these factors and variations relate to patient outcomes. <i>Methods</i>. Comprehensive data from patients who had primary breast cancer surgery from 2010 to 2014 in either a rural or metropolitan location in a single local health district was analysed (<i>n</i> = 686). Records were subset into two rurality groupings based on the postcode in which the patient resided, and the Modified Monash Model (MMM), an Australian system for classifying rurality. Statistical analysis was used to compare rural and metropolitan cohorts on treatments, patient characteristics, timeliness, and outcomes (recurrence and survival). <i>Results</i>. Rural patients had higher mastectomy rates than metropolitan patients (57% vs. 34%, <i>p</i> < 0.001), despite a lack of difference in clinical or demographic factors accounting for such variation. The length of time between treatment pathway stages was consistently longer amongst rural patients (<i>p</i> < 0.01). Rural women also had worse survival outcomes, especially amongst HER2-positive patients who had significantly lower survival (5-year 74% vs 82%; 10-year 49% vs 71%, <i>p</i> < 0.05) than metropolitan HER2-positive patients. <i>Conclusion</i>. This study reveals clinical disparities among rural breast cancer patients, that cannot be explained by demographic and clinical factors alone. Rural patients face lower rates of breast-conserving surgery and treatment delays, attributable to systemic barriers such as limited access to specialist care, high travel costs, and suboptimal care coordination. These findings have important implications for improving equity and collaboration in delivering person-centred breast cancer care.</p>\n </div>","PeriodicalId":56326,"journal":{"name":"Breast Journal","volume":"2024 1","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2024-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/9354395","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast Journal","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/9354395","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
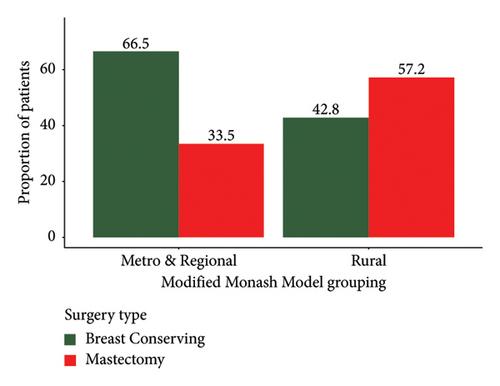
Introduction. Breast cancer management is complex, requiring personalised care from multidisciplinary teams. Research shows that there is unwarranted clinical variation in mastectomy rates between rural and metropolitan patients; that is, variation in treatment which cannot be explained by disease progression or medical necessity. This study aims to determine the clinical and nonclinical factors contributing to any unwarranted variation in breast cancer management in rural patients and to evaluate how these factors and variations relate to patient outcomes. Methods. Comprehensive data from patients who had primary breast cancer surgery from 2010 to 2014 in either a rural or metropolitan location in a single local health district was analysed (n = 686). Records were subset into two rurality groupings based on the postcode in which the patient resided, and the Modified Monash Model (MMM), an Australian system for classifying rurality. Statistical analysis was used to compare rural and metropolitan cohorts on treatments, patient characteristics, timeliness, and outcomes (recurrence and survival). Results. Rural patients had higher mastectomy rates than metropolitan patients (57% vs. 34%, p < 0.001), despite a lack of difference in clinical or demographic factors accounting for such variation. The length of time between treatment pathway stages was consistently longer amongst rural patients (p < 0.01). Rural women also had worse survival outcomes, especially amongst HER2-positive patients who had significantly lower survival (5-year 74% vs 82%; 10-year 49% vs 71%, p < 0.05) than metropolitan HER2-positive patients. Conclusion. This study reveals clinical disparities among rural breast cancer patients, that cannot be explained by demographic and clinical factors alone. Rural patients face lower rates of breast-conserving surgery and treatment delays, attributable to systemic barriers such as limited access to specialist care, high travel costs, and suboptimal care coordination. These findings have important implications for improving equity and collaboration in delivering person-centred breast cancer care.
简介乳腺癌的治疗非常复杂,需要多学科团队提供个性化护理。研究表明,农村和城市患者的乳房切除率存在不必要的临床差异;也就是说,疾病进展或医疗必要性无法解释治疗上的差异。本研究旨在确定导致农村患者乳腺癌治疗出现不必要差异的临床和非临床因素,并评估这些因素和差异与患者预后的关系。研究方法分析了 2010 年至 2014 年期间在一个地方卫生区的农村或城市地区接受乳腺癌初治手术的患者的综合数据(n = 686)。根据患者居住地的邮政编码和澳大利亚乡村分类系统 "改良莫纳什模型"(MMM),将记录分成两个乡村分组。统计分析用于比较乡村组和城市组的治疗方法、患者特征、及时性和结果(复发率和存活率)。结果显示农村患者的乳房切除率高于城市患者(57% vs. 34%, p <0.001),尽管造成这种差异的临床或人口学因素缺乏差异。在农村患者中,治疗路径阶段之间的间隔时间一直较长(p <0.01)。农村妇女的生存率也更低,尤其是HER2阳性患者的生存率(5年74% vs 82%;10年49% vs 71%,p < 0.05)明显低于城市HER2阳性患者。结论。这项研究揭示了农村乳腺癌患者的临床差异,而这些差异不能仅用人口和临床因素来解释。农村患者接受保乳手术和治疗延误的比例较低,这归因于系统性障碍,如获得专科护理的机会有限、旅行成本高以及护理协调不理想。这些发现对改善以人为本的乳腺癌护理的公平性和协作性具有重要意义。
期刊介绍:
The Breast Journal is the first comprehensive, multidisciplinary source devoted exclusively to all facets of research, diagnosis, and treatment of breast disease. The Breast Journal encompasses the latest news and technologies from the many medical specialties concerned with breast disease care in order to address the disease within the context of an integrated breast health care. This editorial philosophy recognizes the special social, sexual, and psychological considerations that distinguish cancer, and breast cancer in particular, from other serious diseases. Topics specifically within the scope of The Breast Journal include:
Risk Factors
Prevention
Early Detection
Diagnosis and Therapy
Psychological Issues
Quality of Life
Biology of Breast Cancer.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
