Jordan S Leyton-Mange, Amanda D Haskell, Kunal Tandon, Andrew C Corsello, Eric Black-Maier, Edward Y Sze, Henry W Sesselberg
{"title":"Protocol modifications reduce risk of delayed pericardial effusions after vein of Marshall ethanol infusion: follow-up from the Maine experience.","authors":"Jordan S Leyton-Mange, Amanda D Haskell, Kunal Tandon, Andrew C Corsello, Eric Black-Maier, Edward Y Sze, Henry W Sesselberg","doi":"10.1007/s10840-024-01842-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While ethanol infusion into the vein of Marshall (VOM) as an adjunct to atrial fibrillation ablation has shown promise, adoption has been limited by the technical expertise required, unclear antiarrhythmic mechanism, and complication risk. Delayed pericardial effusions have been associated with ethanol infusion into the VOM in prior studies. Very little is known about how the procedural approach itself can impact the risk of delayed effusions. We sought to understand the incidence and influence of procedural technique on complications including delayed pericardial effusions from VOM ethanol infusion at a large single medical center.</p><p><strong>Methods: </strong>A total of 275 atrial ablation cases wherein VOM ethanol infusion was attempted were identified from the time of the program's inception in 2019 at Maine Medical Center (Portland, ME) until October of 2023. Cases were classified into phase I cases (early experience) and phase II cases (later experience) based upon temporal programmatic changes in the ethanol dose and infusion rate as well as the use of routine VOM venography. Procedural details and complications were adjudicated from the medical record.</p><p><strong>Results: </strong>The overall VOM ethanol infusion success was 91.4%. Nine complications (3.3%) occurred in eight patients (2.9% of patients). These were more frequent in phase I (5.8%) compared to phase II (1.3%, p = 0.047). This difference was driven by a difference in delayed presentations of tamponade, which occurred in four patients in phase I (3.3%) and in no patients in phase II (0%, p = 0.037). Twelve-month estimated atrial arrhythmia freedom did not differ between groups (73.8% phase I vs 70.4% phase II, p = 0.24).</p><p><strong>Conclusion: </strong>In our single-center experience, adjustments to the procedural approach with lower ethanol infusion rate and dosage, combined with utilizing selective VOM venography, associated with a lowering of complication rates and in particular, delayed pericardial tamponade.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1877-1890"},"PeriodicalIF":2.6000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01842-7","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/24 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: While ethanol infusion into the vein of Marshall (VOM) as an adjunct to atrial fibrillation ablation has shown promise, adoption has been limited by the technical expertise required, unclear antiarrhythmic mechanism, and complication risk. Delayed pericardial effusions have been associated with ethanol infusion into the VOM in prior studies. Very little is known about how the procedural approach itself can impact the risk of delayed effusions. We sought to understand the incidence and influence of procedural technique on complications including delayed pericardial effusions from VOM ethanol infusion at a large single medical center.
Methods: A total of 275 atrial ablation cases wherein VOM ethanol infusion was attempted were identified from the time of the program's inception in 2019 at Maine Medical Center (Portland, ME) until October of 2023. Cases were classified into phase I cases (early experience) and phase II cases (later experience) based upon temporal programmatic changes in the ethanol dose and infusion rate as well as the use of routine VOM venography. Procedural details and complications were adjudicated from the medical record.
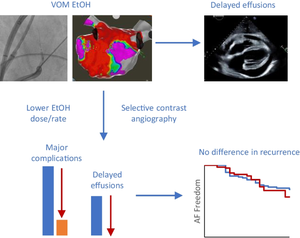
Results: The overall VOM ethanol infusion success was 91.4%. Nine complications (3.3%) occurred in eight patients (2.9% of patients). These were more frequent in phase I (5.8%) compared to phase II (1.3%, p = 0.047). This difference was driven by a difference in delayed presentations of tamponade, which occurred in four patients in phase I (3.3%) and in no patients in phase II (0%, p = 0.037). Twelve-month estimated atrial arrhythmia freedom did not differ between groups (73.8% phase I vs 70.4% phase II, p = 0.24).
Conclusion: In our single-center experience, adjustments to the procedural approach with lower ethanol infusion rate and dosage, combined with utilizing selective VOM venography, associated with a lowering of complication rates and in particular, delayed pericardial tamponade.
背景:虽然将乙醇注入马歇尔静脉(VOM)作为心房颤动消融术的辅助手段已显示出良好的前景,但由于所需的专业技术、抗心律失常机制不明确以及并发症风险等原因,其应用一直受到限制。在之前的研究中,乙醇注入 VOM 与延迟性心包积液有关。关于手术方法本身如何影响延迟渗出的风险,目前所知甚少。我们试图了解一个大型单一医疗中心的手术技术对并发症的发生率和影响,包括VOM乙醇输注引起的延迟性心包积液:从缅因州波特兰市缅因医疗中心(Maine Medical Center)2019 年开始实施该项目到 2023 年 10 月,共确定了 275 例尝试 VOM 乙醇输注的心房消融病例。根据乙醇剂量和输注速度以及常规 VOM 静脉造影的使用情况,将病例分为第一阶段病例(早期经验)和第二阶段病例(后期经验)。手术细节和并发症根据病历进行判定:结果:VOM 乙醇输注的总体成功率为 91.4%。八名患者(占患者总数的 2.9%)出现了九种并发症(3.3%)。第一阶段(5.8%)的并发症发生率高于第二阶段(1.3%,P = 0.047)。这一差异是由延迟出现的血栓栓塞引起的,第一阶段有四名患者(3.3%)出现了血栓栓塞,而第二阶段没有患者出现血栓栓塞(0%,P = 0.037)。12个月的估计房性心律失常自由度在各组之间没有差异(I期73.8% vs II期70.4%,p = 0.24):在我们的单中心经验中,调整手术方法,降低乙醇输注速度和剂量,结合使用选择性 VOM 静脉造影,可降低并发症发生率,尤其是延迟性心包填塞。
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
