Mayra Betancourt Ponce, Eric Schauberger, Ellen Connor, Margo Reeder
{"title":"Delayed hypersensitivity reaction to testosterone cypionate injections","authors":"Mayra Betancourt Ponce, Eric Schauberger, Ellen Connor, Margo Reeder","doi":"10.1111/cod.14624","DOIUrl":null,"url":null,"abstract":"<p>Testicular hypergonadotropic hypogonadism is a disorder characterised by insufficient or absent production of testosterone by the testes in the absence of a hypothalamic or pituitary problem causing delayed or absent puberty. Injections are initially the preferred route of administration of testosterone for puberty induction due to their ability to titrate the small initial doses that are appropriate for puberty induction.<span><sup>1</sup></span></p><p>A 13-year-old male with a history of testicular hypergonadotropic hypogonadism presented to our clinic, reporting a red, itchy rash at the site of his weekly subcutaneous 26 mg dose of testosterone cypionate (200 mg/mL). His first injection was unremarkable; however, a few weeks later, he started developing swelling and pruritic papules at the injection site. The rash developed 8–12 h following injection, lasting 5–7 days before resolution (Figure 1A). Skin prick and intradermal allergy testing for testosterone cypionate (200 mg/mL) were initially negative at their 15-min readings, but the patient developed a delayed positive reaction to the intradermal test the following day (Figure 1B). Patch testing of the excipients, including benzyl benzoate, benzyl alcohol and cottonseed oil, was negative. After switching to testosterone enanthate, the patient was able to resume testosterone therapy.</p><p>Testosterone injections are a common and safe hormone replacement strategy used in different clinical settings, including primary and acquired hypogonadism<span><sup>2</sup></span> and masculinising hormone therapy in transgender individuals.<span><sup>3</sup></span> Short-acting testosterone cypionate and enanthate injections have proven efficacious for puberty induction and are the most used formulations for this purpose.<span><sup>4</sup></span></p><p>Allergic contact dermatitis (ACD) to testosterone is rare and only two cases have been reported.<span><sup>5, 6</sup></span> In these cases, patients raised suspicion of testosterone ACD following reactions to Andropatch® placement and were patch-tested to different testosterone formulations and Andropatch® excipients, including ethanol. Results showed positive reactions to testosterone propionate and undecanoate<span><sup>5</sup></span> in one case and to testosterone enanthate and undecanoate in the other.<span><sup>6</sup></span> To our knowledge, this is the first reported case of a delayed-type hypersensitivity reaction to testosterone cypionate.</p><p>ACD to excipients in injectable testosterone preparations has not been reported. A case of anaphylaxis secondary to benzyl benzoate in testosterone injections was described,<span><sup>7</sup></span> but our patient did not have an immediate reaction and instead developed delayed reactions, consistent with Type IV rather than Type I hypersensitivity reaction. With injections being a common route of administration of testosterone, clinicians should be aware of the rare setting of delayed hypersensitivity to testosterone cypionate, one of the main formulations. In the setting of allergy to testosterone cypionate, alternative injectable formulations can be considered.</p><p>\n <b>Mayra Betancourt Ponce:</b> Writing – original draft; writing – review and editing. <b>Eric Schauberger:</b> Investigation; methodology; validation. <b>Ellen Connor:</b> Investigation; methodology; validation. <b>Margo Reeder:</b> Writing – review and editing; investigation; methodology; validation; supervision.</p><p>The authors declare no conflict of interest.</p>","PeriodicalId":10527,"journal":{"name":"Contact Dermatitis","volume":"91 4","pages":"364-365"},"PeriodicalIF":4.6000,"publicationDate":"2024-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cod.14624","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contact Dermatitis","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cod.14624","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Testicular hypergonadotropic hypogonadism is a disorder characterised by insufficient or absent production of testosterone by the testes in the absence of a hypothalamic or pituitary problem causing delayed or absent puberty. Injections are initially the preferred route of administration of testosterone for puberty induction due to their ability to titrate the small initial doses that are appropriate for puberty induction.1
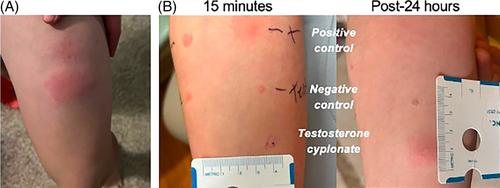
A 13-year-old male with a history of testicular hypergonadotropic hypogonadism presented to our clinic, reporting a red, itchy rash at the site of his weekly subcutaneous 26 mg dose of testosterone cypionate (200 mg/mL). His first injection was unremarkable; however, a few weeks later, he started developing swelling and pruritic papules at the injection site. The rash developed 8–12 h following injection, lasting 5–7 days before resolution (Figure 1A). Skin prick and intradermal allergy testing for testosterone cypionate (200 mg/mL) were initially negative at their 15-min readings, but the patient developed a delayed positive reaction to the intradermal test the following day (Figure 1B). Patch testing of the excipients, including benzyl benzoate, benzyl alcohol and cottonseed oil, was negative. After switching to testosterone enanthate, the patient was able to resume testosterone therapy.
Testosterone injections are a common and safe hormone replacement strategy used in different clinical settings, including primary and acquired hypogonadism2 and masculinising hormone therapy in transgender individuals.3 Short-acting testosterone cypionate and enanthate injections have proven efficacious for puberty induction and are the most used formulations for this purpose.4
Allergic contact dermatitis (ACD) to testosterone is rare and only two cases have been reported.5, 6 In these cases, patients raised suspicion of testosterone ACD following reactions to Andropatch® placement and were patch-tested to different testosterone formulations and Andropatch® excipients, including ethanol. Results showed positive reactions to testosterone propionate and undecanoate5 in one case and to testosterone enanthate and undecanoate in the other.6 To our knowledge, this is the first reported case of a delayed-type hypersensitivity reaction to testosterone cypionate.
ACD to excipients in injectable testosterone preparations has not been reported. A case of anaphylaxis secondary to benzyl benzoate in testosterone injections was described,7 but our patient did not have an immediate reaction and instead developed delayed reactions, consistent with Type IV rather than Type I hypersensitivity reaction. With injections being a common route of administration of testosterone, clinicians should be aware of the rare setting of delayed hypersensitivity to testosterone cypionate, one of the main formulations. In the setting of allergy to testosterone cypionate, alternative injectable formulations can be considered.
Mayra Betancourt Ponce: Writing – original draft; writing – review and editing. Eric Schauberger: Investigation; methodology; validation. Ellen Connor: Investigation; methodology; validation. Margo Reeder: Writing – review and editing; investigation; methodology; validation; supervision.
期刊介绍:
Contact Dermatitis is designed primarily as a journal for clinicians who are interested in various aspects of environmental dermatitis. This includes both allergic and irritant (toxic) types of contact dermatitis, occupational (industrial) dermatitis and consumers" dermatitis from such products as cosmetics and toiletries. The journal aims at promoting and maintaining communication among dermatologists, industrial physicians, allergists and clinical immunologists, as well as chemists and research workers involved in industry and the production of consumer goods. Papers are invited on clinical observations, diagnosis and methods of investigation of patients, therapeutic measures, organisation and legislation relating to the control of occupational and consumers".



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
