Leandro F. Pippa, Valvanera Vozmediano, Lieke Mitrov-Winkelmolen, Daan Touw, Amira Soliman, Rodrigo Cristofoletti, Wilson Salgado Junior, Natalia Valadares de Moraes
{"title":"Impact of obesity and roux-en-Y gastric bypass on the pharmacokinetics of (R)- and (S)-omeprazole and intragastric pH","authors":"Leandro F. Pippa, Valvanera Vozmediano, Lieke Mitrov-Winkelmolen, Daan Touw, Amira Soliman, Rodrigo Cristofoletti, Wilson Salgado Junior, Natalia Valadares de Moraes","doi":"10.1002/psp4.13189","DOIUrl":null,"url":null,"abstract":"<p>This study employed physiologically-based pharmacokinetic–pharmacodynamics (PBPK/PD) modeling to predict the effect of obesity and gastric bypass surgery on the pharmacokinetics and intragastric pH following omeprazole treatment. The simulated plasma concentrations closely matched the observed data from non-obese, morbidly obese, and post-gastric bypass populations. Obesity significantly reduces CYP3A4 and CYP2C19 activities, as reflected by the metabolic ratio [omeprazole sulphone]/[omeprazole] and [5-hydroxy-omeprazole]/[omeprazole]. The morbidly obese model accounted for the down-regulation of CYP2C19 and CYP3A4 to recapitulate the observed data. Sensitivity analysis showed that intestinal CYP3A4, gastric pH, small intestine bypass, and the delay in bile release do not have a major influence on omeprazole exposure. Hepatic CYP3A4 had a significant impact on the AUC of (<i>S</i>)-omeprazole, while hepatic CYP2C19 affected both (<i>R</i>)- and (<i>S</i>)-omeprazole AUC. After gastric bypass surgery, the activity of CYP3A4 and CYP2C19 is restored. The PBPK model was linked to a mechanism-based PD model to assess the effect of omeprazole on intragastric pH. Following 40 mg omeprazole, the mean intragastric pH was 4.3, 4.6, and 6.6 in non-obese, obese, and post-gastric bypass populations, and the daily time with pH >4 was 14.7, 16.4, and 24 h. Our PBPK/PD approach provides a comprehensive understating of the impact of obesity and weight loss on CYP3A4 and CYP2C19 activity and omeprazole pharmacokinetics. Given that simulated intragastric pH is relatively high in post-RYGB patients, irrespective of the dose of omeprazole, additional clinical outcomes are imperative to assess the effect of proton pump inhibitor in preventing marginal ulcers in this population.</p>","PeriodicalId":10774,"journal":{"name":"CPT: Pharmacometrics & Systems Pharmacology","volume":"13 9","pages":"1528-1541"},"PeriodicalIF":3.0000,"publicationDate":"2024-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/psp4.13189","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CPT: Pharmacometrics & Systems Pharmacology","FirstCategoryId":"3","ListUrlMain":"https://ascpt.onlinelibrary.wiley.com/doi/10.1002/psp4.13189","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
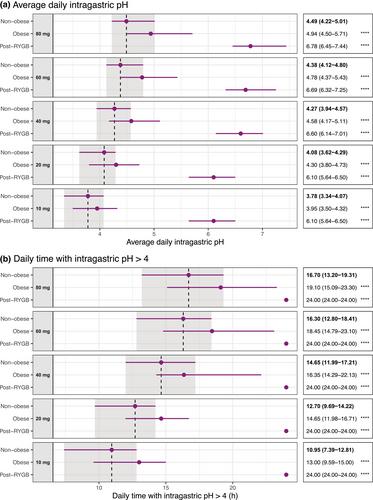
This study employed physiologically-based pharmacokinetic–pharmacodynamics (PBPK/PD) modeling to predict the effect of obesity and gastric bypass surgery on the pharmacokinetics and intragastric pH following omeprazole treatment. The simulated plasma concentrations closely matched the observed data from non-obese, morbidly obese, and post-gastric bypass populations. Obesity significantly reduces CYP3A4 and CYP2C19 activities, as reflected by the metabolic ratio [omeprazole sulphone]/[omeprazole] and [5-hydroxy-omeprazole]/[omeprazole]. The morbidly obese model accounted for the down-regulation of CYP2C19 and CYP3A4 to recapitulate the observed data. Sensitivity analysis showed that intestinal CYP3A4, gastric pH, small intestine bypass, and the delay in bile release do not have a major influence on omeprazole exposure. Hepatic CYP3A4 had a significant impact on the AUC of (S)-omeprazole, while hepatic CYP2C19 affected both (R)- and (S)-omeprazole AUC. After gastric bypass surgery, the activity of CYP3A4 and CYP2C19 is restored. The PBPK model was linked to a mechanism-based PD model to assess the effect of omeprazole on intragastric pH. Following 40 mg omeprazole, the mean intragastric pH was 4.3, 4.6, and 6.6 in non-obese, obese, and post-gastric bypass populations, and the daily time with pH >4 was 14.7, 16.4, and 24 h. Our PBPK/PD approach provides a comprehensive understating of the impact of obesity and weight loss on CYP3A4 and CYP2C19 activity and omeprazole pharmacokinetics. Given that simulated intragastric pH is relatively high in post-RYGB patients, irrespective of the dose of omeprazole, additional clinical outcomes are imperative to assess the effect of proton pump inhibitor in preventing marginal ulcers in this population.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
