Comparison of anticoagulation control and outcomes between usual medical care and pharmacist-led anticoagulation service in ambulatory patients taking warfarin at tertiary hospital in Ethiopia: a quasi-experimental study.
{"title":"Comparison of anticoagulation control and outcomes between usual medical care and pharmacist-led anticoagulation service in ambulatory patients taking warfarin at tertiary hospital in Ethiopia: a quasi-experimental study.","authors":"Tamrat Assefa Tadesse, Amha Gebremedhin, Dejuma Yadeta, Legese Chelkeba, Teferi Gedif Fenta","doi":"10.1186/s40780-024-00355-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We aimed to compare anticoagulation control and outcomes between usual medical care (UMC) and pharmacist-led anticoagulation services (PLAS) in patients receiving warfarin at the Tikur Anbessa Specialized Hospital (TASH), Addis Ababa, Ethiopia.</p><p><strong>Methods: </strong>A quasi-experimental study was conducted, including 350 (66.7%) and 175 (33.3%) patients from the UMC and PLAS groups, respectively, from 525 patients. The time in therapeutic range (TTR) was determined using the Rosendaal method, with a TTR ≥ 65% set as the cut-off for optimal anticoagulation. The two-sample Wilcoxon rank-sum (Mann-Whitney U) test was used to compare continuous variables between groups. Categorical variables were compared between groups using Pearson's chi-square test or Fisher's exact test. Logistic regression and negative binomial regression analyses were conducted to identify the factors associated with suboptimal TTR and secondary outcomes, respectively, at the p values < 0.05, and 95% confidence interval (CI).</p><p><strong>Results: </strong>Compared with the UMC group, the patients in the PLAC group showed a significantly higher median (IQR) TTR [60.89% (43.5-74.69%) vs. 53.65% (33.92-69.14%), p < 0.001]. A significantly higher optimal TTR (≥ 65%) was achieved in the PLAC group (41.7% vs. 31.7%) than in the UMC group (p = 0.002). The odds of having a poor TTR were reduced by 43% (AOR = 0.57, 95% CI = 0.36-0.88, p = 0.01) among patients in the PLAC group compared to those in the UMC group. There were no statistically significant differences in the secondary outcomes between the groups, except for all-cause emergency visits (p = 0.003). The incidence of bleeding events decreased by 3% (IRR = 0.97, 95% CI = 0.96-0.99, p < 0.001) for every increase in INR monitoring frequency. The incidence of thromboembolic events increased by a factor of 15.13 (IRR = 15.13, 95% CI = 1.47-155.52, p = 0.02) among patients with a high-risk CHA<sub>2</sub>DS<sub>2</sub>-VASc score compared with those with a moderate score.</p><p><strong>Conclusion: </strong>Patients in the PLAC group had a significantly higher median TTR than those in the UMC group did. There were no statistically significant differences in the secondary outcomes between the groups, except for fewer all-cause emergency department visits in the PLAC group.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":"10 1","pages":"32"},"PeriodicalIF":1.2000,"publicationDate":"2024-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11202342/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-024-00355-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We aimed to compare anticoagulation control and outcomes between usual medical care (UMC) and pharmacist-led anticoagulation services (PLAS) in patients receiving warfarin at the Tikur Anbessa Specialized Hospital (TASH), Addis Ababa, Ethiopia.
Methods: A quasi-experimental study was conducted, including 350 (66.7%) and 175 (33.3%) patients from the UMC and PLAS groups, respectively, from 525 patients. The time in therapeutic range (TTR) was determined using the Rosendaal method, with a TTR ≥ 65% set as the cut-off for optimal anticoagulation. The two-sample Wilcoxon rank-sum (Mann-Whitney U) test was used to compare continuous variables between groups. Categorical variables were compared between groups using Pearson's chi-square test or Fisher's exact test. Logistic regression and negative binomial regression analyses were conducted to identify the factors associated with suboptimal TTR and secondary outcomes, respectively, at the p values < 0.05, and 95% confidence interval (CI).
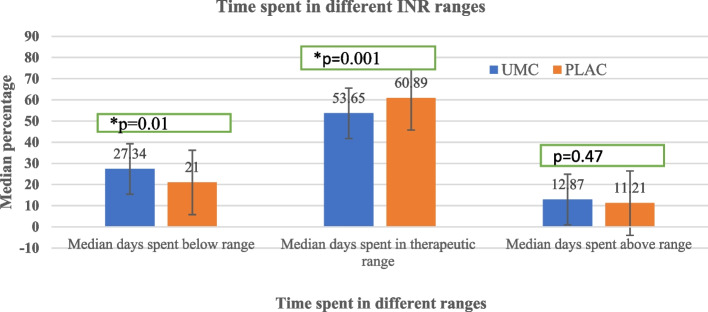
Results: Compared with the UMC group, the patients in the PLAC group showed a significantly higher median (IQR) TTR [60.89% (43.5-74.69%) vs. 53.65% (33.92-69.14%), p < 0.001]. A significantly higher optimal TTR (≥ 65%) was achieved in the PLAC group (41.7% vs. 31.7%) than in the UMC group (p = 0.002). The odds of having a poor TTR were reduced by 43% (AOR = 0.57, 95% CI = 0.36-0.88, p = 0.01) among patients in the PLAC group compared to those in the UMC group. There were no statistically significant differences in the secondary outcomes between the groups, except for all-cause emergency visits (p = 0.003). The incidence of bleeding events decreased by 3% (IRR = 0.97, 95% CI = 0.96-0.99, p < 0.001) for every increase in INR monitoring frequency. The incidence of thromboembolic events increased by a factor of 15.13 (IRR = 15.13, 95% CI = 1.47-155.52, p = 0.02) among patients with a high-risk CHA2DS2-VASc score compared with those with a moderate score.
Conclusion: Patients in the PLAC group had a significantly higher median TTR than those in the UMC group did. There were no statistically significant differences in the secondary outcomes between the groups, except for fewer all-cause emergency department visits in the PLAC group.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
