V. Le Cam Duchez, C. Ternisien, E. A. Guery, V. Eschwège, E. Jeanpierre, C. Nougier, V. Proulle, A. Stepanian, M. Tuffigo, R. Marlu, C. Pouplard
{"title":"Cross-reactivity of human anti-FVIII antibodies to porcine rFVIII: French field study to validate the modified Nijmegen method","authors":"V. Le Cam Duchez, C. Ternisien, E. A. Guery, V. Eschwège, E. Jeanpierre, C. Nougier, V. Proulle, A. Stepanian, M. Tuffigo, R. Marlu, C. Pouplard","doi":"10.1111/ijlh.14331","DOIUrl":null,"url":null,"abstract":"<p>Acquired hemophilia A (AHA) is a rare autoimmune bleeding disorder resulting from the development of inhibitory autoantibodies against the circulating factor VIII (FVIII:C). It occurs in patients without a family or personal history of bleeding.<span><sup>1</sup></span> AHA incidence is approximately 1.5 cases/million/year<span><sup>2</sup></span> and is idiopathic in about 50% of cases AHA.<span><sup>3</sup></span> AHA is biologically characterized by an isolated deficiency of coagulation factor VIII (FVIII:C) secondary to autoantibodies targeting specific epitopes that cause neutralization and/or accelerated clearance of FVIII from the plasma (auto-FVIII Abs).<span><sup>4</sup></span></p><p>More often, diagnosis is triggered by a bleeding event<span><sup>3</sup></span> and confirmed by laboratory data: a decreased level of FVIII:C, usually lower than 30% and the presence of anti-FVIII antibodies with a titer >0.6 Bethesda Unit/mL.<span><sup>5</sup></span> In case of severe bleeding event, an hemostatic treatment with bypassing agents, including recombinant Factor VIIa (rFVIIa) or activated prothrombin complex concentrates (aPCCs), is recommended.<span><sup>6, 7</sup></span> More recently, the recommendations for hemostatic treatment in AHA included a “new” treatment, susoctocog alfa (Obizur®): a recombinant porcine FVIII (rpFVIII).<span><sup>5</sup></span> This recombinant and highly purified protein has comparable biochemical and hemostatic properties to plasma-derived porcine factor VIII, but much lower risks of infection and toxicity. This recombinant anti-hemophilic factor porcine sequence (rpFVIII) is a B-domain deleted FVIII produced in baby hamster kidney (BHK) cells. Susoctocog alfa was approved for treatment of bleeding episodes in AHA in October 2014 in the United States and in November 2015 in Europe. Nevertheless, as recommended in the summary of product characteristics (SmPC), prior to any treatment with rpFVIII, it is necessary to test the cross-reactivity of auto-FVIII Abs with rpFVIII. A close monitoring of rpFVIII activity during treatment is also recommended.<span><sup>5</sup></span> However, some questions remain concerning this laboratory assessment. The method used for the titration of anti-porcine FVIII inhibitors is comparable to that conventionally used in our laboratories. However, SmPC notifies that the patient's plasma must be incubated with plasma titrated for porcine factor-VIII instead of the normal human plasma usually used. In addition, the reference/control should be obtained by diluting rpFVIII in plasma deficient in factor VIII and not in imidazole buffer, as usually carried out.<span><sup>8</sup></span></p><p>The aim objective of this study is first to validate in a field study the modified Nijmegen method used in our laboratories for the anti-rpFVIII titration. Ten French laboratories participated to this study and each used its local own automated, aPTT reagent and FVIII deficient plasma to perform the FVIII one-stage assay (OSA).</p><p>We first compared the stability of rpFVIII after 2 h-incubation at 37°C in buffered FVIII-deficient plasma (FVIII-DP) or in imidazole buffer (IB). Recombinant pFVIII was supplied by Takeda and was first reconstituted with 1 mL of distilled water, then diluted (1/11) in buffered factor VIII-DP containing von Willebrand factor (Siemens) to obtain a concentration close to 100 IU/dL. Two different volume-to-volume mixtures were then prepared: Mixture 1: rpFVIII at 100 IU/dL + FVIII-DP and Mixture 2: rpFVIII at 100 IU/dL + IB. Factor VIII activity was measured, with a FVIII assay calibrated with NIBSC calibrator, immediately and after 2 h incubation at 37°C. Procedure was repeated in each participant laboratory three times (i.e., on three different days) resulting in three assay runs. After 2 h incubation, a decrease in rpFVIII activity was observed in each mixture and the mean differences ± standard deviation (SD) were minus 1.9 ± 3.4 IU/dL and minus 1.8 ± 2.9 IU/dL when standard rpFVIII was diluted in FVIII-deficient plasma or Imidazole buffer, respectively (Figure 1) without statistical difference between these variations (<i>t</i>-test: <i>p</i> = 0.938).</p><p>We then applied the modified Nijmegen method to assess the cross-reactivity of plasma from patients with congenital hemophilia A with inhibitors (PWA) or AHA. In this step, each sample was systematically tested in two different centers (paired-centers described in Table 1). Thirty eight samples from 26 patients with AHA and 12 samples from 7 patients with hemophilia A (PWA) with circulating anti-FVIII antibodies were tested. In each laboratory, plasma samples dilutions were performed with IB instead of FVIII-DP. To evaluate the inter-laboratory variations, a set of 10 samples were systematically sent to two different laboratories. In addition, a control sample (weak human FVIII inhibitor plasma control, Cryopep, Montpellier, France) was tested in each run. Anti-rpFVIII titration was performed in each center using the following method: prior to testing, plasma samples were incubated for 30 min at 58°C as recommended by Verbruggen et al.<span><sup>9</sup></span> and centrifuged for 10–15 min at 2500 g. Recombinant pFVIII (substrate) was reconstituted with 1 mL of distilled water and diluted 1:11 in FVIII-deficient plasma containing VWF to obtain an activity close to 100 IU/dL. For anti-rpFVIII titration, each laboratory used its own aPTT reagent and calibration curves. Several dilutions of the samples with IB were systematically performed (1:1, 1:2, 1:5, 1:10, 1:20, and 1:30). Results of rpFVIII antibodies titration of the 50 plasmas selected are shown in Table 1, and the median results obtained in the two different laboratories are shown in Figure 2 according to the population studied. We did not observed cross-reactivity to rpFVIII with the FVIII inhibitor control plasma (data none show). In 25/50 plasma samples tested, no cross-reactivity against rpFVIII was detected in either laboratory. The mean anti-hFVIII titer of these 25 samples was 14.9 BU/mL [range: 0.7–112 BU/mL]. In contrast, cross-reactivity with rpFVIII was detected by both laboratories in 19/50 samples with a mean titer of 8.5 BU/mL [range: 1.0–93.3 BU/mL]. The mean anti-hFVIII titer of these 19 samples was 37.6 BU/mL [range: 1–320 BU/mL]. Among these 19 samples, 10 came from AHA patients and 9 came from PWA with inhibitors. Cross-reactivity was clearly detected in 26% (10/38) of samples from AHA patients versus 75% (9/12) of samples from PWA with inhibitors. However, several samples from one patient were tested, and if we analyze the frequency of cross-reactivity according to patients, it was detected in 7/26 (27%) patients with AHA versus 4/7 (57%) PWA with inhibitors.</p><p>Discrepancies between laboratories were reported in six samples (CO04, TOP1, NA12, RO08, LI01, and LI03) with a mean anti-rpFVIII titer equal to 0.9 BU/mL [range 0.6–1.36 BU/mL]. Among these, five were from AHA patients with probably a type 2 kinetic, which is more frequent in AHA.<span><sup>6</sup></span> In addition, due to the multiplicity of reagents/methods used to measure residual FVIII, the concordance of results between laboratories can be relatively poor. Cross-reactivity was therefore considered positive in 16 of the 38 AHA samples (42%) but a cross-reactivity against rpFVIII above 20 BU/mL was detected in only one sample from a PWA with a titer of anti-hFVIII inhibitor at 57 BU/mL.</p><p>In conclusion, our field study demonstrated the feasibility of using imidazole buffer to detect anti-rpFVIII antibodies, and confirmed the absence of impact of aPTT reagent and calibration curves on the method.<span><sup>10</sup></span> The United Kingdom Haemophilia Centre Doctor's organisation guidelines<span><sup>11</sup></span> recommended to use “a locally verified one-stage APTT-based assays calibrated against plasma standards to monitor rpFVIII” and a modified Bethesda assay using rpFVIII as the substrate without precision about the use of FVIII deficient plasma or imidazole buffer. A specific calibration curve using rpFVIII has been recommended by Novembrino to determine recovery as well as FVIII-DP containing VWF both for diluting standard rpFVIII and for performing OSA.<span><sup>12</sup></span></p><p>Our study confirmed a frequency of cross-reactivity with rpFVIII close to 40% in AHAs. However, high cross-reactivity, above 20 BU/mL, contraindicating treatment, is rare and has not been observed in our AHA population.</p><p>All authors contributed to perform analysis of this study. V. Le Cam Duchez, C. Ternisien, and C. Pouplard contributed to the design of study and wrote the manuscript. All authors read and approved the final manuscript.</p><p>This work was supported by Takeda.</p>","PeriodicalId":14120,"journal":{"name":"International Journal of Laboratory Hematology","volume":"46 6","pages":"1118-1122"},"PeriodicalIF":2.3000,"publicationDate":"2024-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ijlh.14331","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Laboratory Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ijlh.14331","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Acquired hemophilia A (AHA) is a rare autoimmune bleeding disorder resulting from the development of inhibitory autoantibodies against the circulating factor VIII (FVIII:C). It occurs in patients without a family or personal history of bleeding.1 AHA incidence is approximately 1.5 cases/million/year2 and is idiopathic in about 50% of cases AHA.3 AHA is biologically characterized by an isolated deficiency of coagulation factor VIII (FVIII:C) secondary to autoantibodies targeting specific epitopes that cause neutralization and/or accelerated clearance of FVIII from the plasma (auto-FVIII Abs).4
More often, diagnosis is triggered by a bleeding event3 and confirmed by laboratory data: a decreased level of FVIII:C, usually lower than 30% and the presence of anti-FVIII antibodies with a titer >0.6 Bethesda Unit/mL.5 In case of severe bleeding event, an hemostatic treatment with bypassing agents, including recombinant Factor VIIa (rFVIIa) or activated prothrombin complex concentrates (aPCCs), is recommended.6, 7 More recently, the recommendations for hemostatic treatment in AHA included a “new” treatment, susoctocog alfa (Obizur®): a recombinant porcine FVIII (rpFVIII).5 This recombinant and highly purified protein has comparable biochemical and hemostatic properties to plasma-derived porcine factor VIII, but much lower risks of infection and toxicity. This recombinant anti-hemophilic factor porcine sequence (rpFVIII) is a B-domain deleted FVIII produced in baby hamster kidney (BHK) cells. Susoctocog alfa was approved for treatment of bleeding episodes in AHA in October 2014 in the United States and in November 2015 in Europe. Nevertheless, as recommended in the summary of product characteristics (SmPC), prior to any treatment with rpFVIII, it is necessary to test the cross-reactivity of auto-FVIII Abs with rpFVIII. A close monitoring of rpFVIII activity during treatment is also recommended.5 However, some questions remain concerning this laboratory assessment. The method used for the titration of anti-porcine FVIII inhibitors is comparable to that conventionally used in our laboratories. However, SmPC notifies that the patient's plasma must be incubated with plasma titrated for porcine factor-VIII instead of the normal human plasma usually used. In addition, the reference/control should be obtained by diluting rpFVIII in plasma deficient in factor VIII and not in imidazole buffer, as usually carried out.8
The aim objective of this study is first to validate in a field study the modified Nijmegen method used in our laboratories for the anti-rpFVIII titration. Ten French laboratories participated to this study and each used its local own automated, aPTT reagent and FVIII deficient plasma to perform the FVIII one-stage assay (OSA).
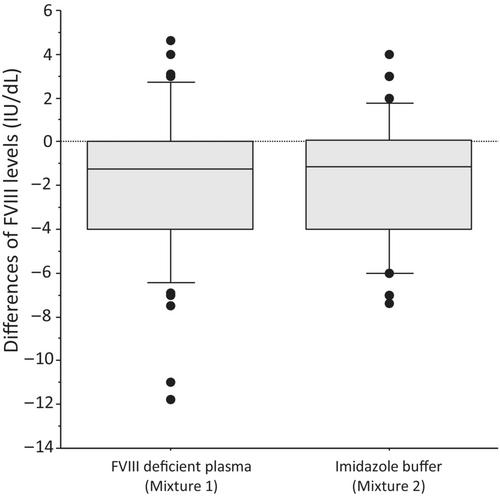
We first compared the stability of rpFVIII after 2 h-incubation at 37°C in buffered FVIII-deficient plasma (FVIII-DP) or in imidazole buffer (IB). Recombinant pFVIII was supplied by Takeda and was first reconstituted with 1 mL of distilled water, then diluted (1/11) in buffered factor VIII-DP containing von Willebrand factor (Siemens) to obtain a concentration close to 100 IU/dL. Two different volume-to-volume mixtures were then prepared: Mixture 1: rpFVIII at 100 IU/dL + FVIII-DP and Mixture 2: rpFVIII at 100 IU/dL + IB. Factor VIII activity was measured, with a FVIII assay calibrated with NIBSC calibrator, immediately and after 2 h incubation at 37°C. Procedure was repeated in each participant laboratory three times (i.e., on three different days) resulting in three assay runs. After 2 h incubation, a decrease in rpFVIII activity was observed in each mixture and the mean differences ± standard deviation (SD) were minus 1.9 ± 3.4 IU/dL and minus 1.8 ± 2.9 IU/dL when standard rpFVIII was diluted in FVIII-deficient plasma or Imidazole buffer, respectively (Figure 1) without statistical difference between these variations (t-test: p = 0.938).
We then applied the modified Nijmegen method to assess the cross-reactivity of plasma from patients with congenital hemophilia A with inhibitors (PWA) or AHA. In this step, each sample was systematically tested in two different centers (paired-centers described in Table 1). Thirty eight samples from 26 patients with AHA and 12 samples from 7 patients with hemophilia A (PWA) with circulating anti-FVIII antibodies were tested. In each laboratory, plasma samples dilutions were performed with IB instead of FVIII-DP. To evaluate the inter-laboratory variations, a set of 10 samples were systematically sent to two different laboratories. In addition, a control sample (weak human FVIII inhibitor plasma control, Cryopep, Montpellier, France) was tested in each run. Anti-rpFVIII titration was performed in each center using the following method: prior to testing, plasma samples were incubated for 30 min at 58°C as recommended by Verbruggen et al.9 and centrifuged for 10–15 min at 2500 g. Recombinant pFVIII (substrate) was reconstituted with 1 mL of distilled water and diluted 1:11 in FVIII-deficient plasma containing VWF to obtain an activity close to 100 IU/dL. For anti-rpFVIII titration, each laboratory used its own aPTT reagent and calibration curves. Several dilutions of the samples with IB were systematically performed (1:1, 1:2, 1:5, 1:10, 1:20, and 1:30). Results of rpFVIII antibodies titration of the 50 plasmas selected are shown in Table 1, and the median results obtained in the two different laboratories are shown in Figure 2 according to the population studied. We did not observed cross-reactivity to rpFVIII with the FVIII inhibitor control plasma (data none show). In 25/50 plasma samples tested, no cross-reactivity against rpFVIII was detected in either laboratory. The mean anti-hFVIII titer of these 25 samples was 14.9 BU/mL [range: 0.7–112 BU/mL]. In contrast, cross-reactivity with rpFVIII was detected by both laboratories in 19/50 samples with a mean titer of 8.5 BU/mL [range: 1.0–93.3 BU/mL]. The mean anti-hFVIII titer of these 19 samples was 37.6 BU/mL [range: 1–320 BU/mL]. Among these 19 samples, 10 came from AHA patients and 9 came from PWA with inhibitors. Cross-reactivity was clearly detected in 26% (10/38) of samples from AHA patients versus 75% (9/12) of samples from PWA with inhibitors. However, several samples from one patient were tested, and if we analyze the frequency of cross-reactivity according to patients, it was detected in 7/26 (27%) patients with AHA versus 4/7 (57%) PWA with inhibitors.
Discrepancies between laboratories were reported in six samples (CO04, TOP1, NA12, RO08, LI01, and LI03) with a mean anti-rpFVIII titer equal to 0.9 BU/mL [range 0.6–1.36 BU/mL]. Among these, five were from AHA patients with probably a type 2 kinetic, which is more frequent in AHA.6 In addition, due to the multiplicity of reagents/methods used to measure residual FVIII, the concordance of results between laboratories can be relatively poor. Cross-reactivity was therefore considered positive in 16 of the 38 AHA samples (42%) but a cross-reactivity against rpFVIII above 20 BU/mL was detected in only one sample from a PWA with a titer of anti-hFVIII inhibitor at 57 BU/mL.
In conclusion, our field study demonstrated the feasibility of using imidazole buffer to detect anti-rpFVIII antibodies, and confirmed the absence of impact of aPTT reagent and calibration curves on the method.10 The United Kingdom Haemophilia Centre Doctor's organisation guidelines11 recommended to use “a locally verified one-stage APTT-based assays calibrated against plasma standards to monitor rpFVIII” and a modified Bethesda assay using rpFVIII as the substrate without precision about the use of FVIII deficient plasma or imidazole buffer. A specific calibration curve using rpFVIII has been recommended by Novembrino to determine recovery as well as FVIII-DP containing VWF both for diluting standard rpFVIII and for performing OSA.12
Our study confirmed a frequency of cross-reactivity with rpFVIII close to 40% in AHAs. However, high cross-reactivity, above 20 BU/mL, contraindicating treatment, is rare and has not been observed in our AHA population.
All authors contributed to perform analysis of this study. V. Le Cam Duchez, C. Ternisien, and C. Pouplard contributed to the design of study and wrote the manuscript. All authors read and approved the final manuscript.
期刊介绍:
The International Journal of Laboratory Hematology provides a forum for the communication of new developments, research topics and the practice of laboratory haematology.
The journal publishes invited reviews, full length original articles, and correspondence.
The International Journal of Laboratory Hematology is the official journal of the International Society for Laboratory Hematology, which addresses the following sub-disciplines: cellular analysis, flow cytometry, haemostasis and thrombosis, molecular diagnostics, haematology informatics, haemoglobinopathies, point of care testing, standards and guidelines.
The journal was launched in 2006 as the successor to Clinical and Laboratory Hematology, which was first published in 1979. An active and positive editorial policy ensures that work of a high scientific standard is reported, in order to bridge the gap between practical and academic aspects of laboratory haematology.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
