{"title":"[Cost comparison of conservative vs. surgical treatment of chronic lymphedema].","authors":"Rima Nuwayhid, Stefan Langer, Nikolaus von Dercks","doi":"10.1007/s00104-024-02123-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lymphedema is primarily treated conservatively using complex physical decongestion treatment (CDT). Lymphovenous anastomosis (LVA), vascularized lymph node transplantation (VLNT) and liposuction are available as surgical treatment methods; however, reimbursement in the diagnosis-related groups (DRG) system is sometimes inadequate or only possible following an individual application. The costs of these relatively new surgical procedures have not yet been set in relation to those of CDT.</p><p><strong>Method: </strong>The costs of conservative treatment were determined in accordance with the guidelines. The costs for LVA, VLNT and liposuction of the upper and lower extremities were estimated on the basis of the DRG reimbursement per case and the expected reduction in conservative measures according to current knowledge. The annual treatment costs were then compared.</p><p><strong>Results: </strong>The annual treatment costs of LVA and VLNT are already lower than conservative treatment alone in the second postoperative year. Liposuction reaches this point in the 6th (upper extremity) or 47th postoperative year (lower extremity).</p><p><strong>Conclusion: </strong>The evidence for the positive effects of lymphatic surgery is still limited; however, it is recognizable that the curative surgical approach can significantly reduce the treatment costs and improve the quality of life of lymphedema patients; however, there is a lack of adequate reflection of the surgical effort in the reimbursement.</p>","PeriodicalId":72588,"journal":{"name":"Chirurgie (Heidelberg, Germany)","volume":" ","pages":"41-47"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11729079/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chirurgie (Heidelberg, Germany)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00104-024-02123-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Lymphedema is primarily treated conservatively using complex physical decongestion treatment (CDT). Lymphovenous anastomosis (LVA), vascularized lymph node transplantation (VLNT) and liposuction are available as surgical treatment methods; however, reimbursement in the diagnosis-related groups (DRG) system is sometimes inadequate or only possible following an individual application. The costs of these relatively new surgical procedures have not yet been set in relation to those of CDT.
Method: The costs of conservative treatment were determined in accordance with the guidelines. The costs for LVA, VLNT and liposuction of the upper and lower extremities were estimated on the basis of the DRG reimbursement per case and the expected reduction in conservative measures according to current knowledge. The annual treatment costs were then compared.
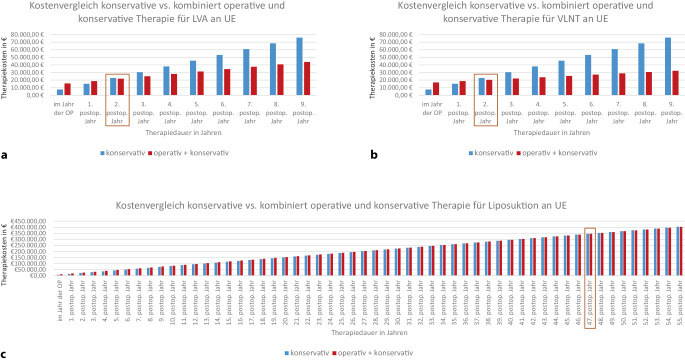
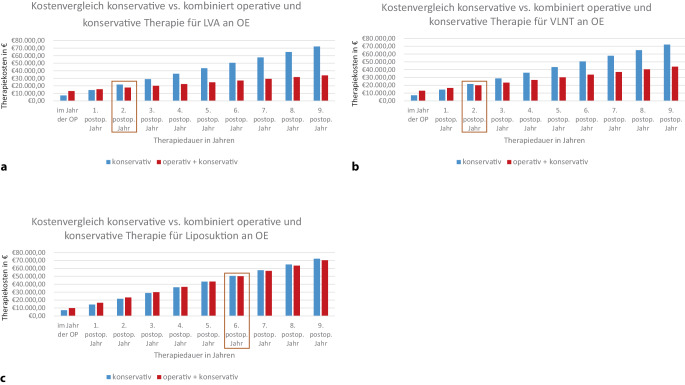
Results: The annual treatment costs of LVA and VLNT are already lower than conservative treatment alone in the second postoperative year. Liposuction reaches this point in the 6th (upper extremity) or 47th postoperative year (lower extremity).
Conclusion: The evidence for the positive effects of lymphatic surgery is still limited; however, it is recognizable that the curative surgical approach can significantly reduce the treatment costs and improve the quality of life of lymphedema patients; however, there is a lack of adequate reflection of the surgical effort in the reimbursement.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
