Matthias Görges, Jonath Sujan, Nicholas C West, Rama Syamala Sreepada, Michael D Wood, Beth A Payne, Swati Shetty, Jean P Gelinas, Ainsley M Sutherland
{"title":"Postsurgical Pain Risk Stratification to Enhance Pain Management Workflow in Adult Patients: Design, Implementation, and Pilot Evaluation.","authors":"Matthias Görges, Jonath Sujan, Nicholas C West, Rama Syamala Sreepada, Michael D Wood, Beth A Payne, Swati Shetty, Jean P Gelinas, Ainsley M Sutherland","doi":"10.2196/54926","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Exposure to opioids after surgery is the initial contact for some people who develop chronic opioid use disorder. Hence, effective postoperative pain management, with less reliance on opioids, is critical. The Perioperative Opioid Quality Improvement (POQI) program developed (1) a digital health platform leveraging patient-survey-reported risk factors and (2) a postsurgical pain risk stratification algorithm to personalize perioperative care by integrating several commercially available digital health solutions into a combined platform. Development was reduced in scope by the COVID-19 pandemic.</p><p><strong>Objective: </strong>This pilot study aims to assess the screening performance of the risk algorithm, quantify the use of the POQI platform, and evaluate clinicians' and patients' perceptions of its utility and benefit.</p><p><strong>Methods: </strong>A POQI platform prototype was implemented in a quality improvement initiative at a Canadian tertiary care center and evaluated from January to September 2022. After surgical booking, a preliminary risk stratification algorithm was applied to health history questionnaire responses. The estimated risk guided the patient assignment to a care pathway based on low or high risk for persistent pain and opioid use. Demographic, procedural, and medication administration data were extracted retrospectively from the electronic medical record. Postoperative inpatient opioid use of >90 morphine milligram equivalents per day was the outcome used to assess algorithm performance. Data were summarized and compared between the low- and high-risk groups. POQI use was assessed by completed surveys on postoperative days 7, 14, 30, 60, 90, and 120. Semistructured patient and clinician interviews provided qualitative feedback on the platform.</p><p><strong>Results: </strong>Overall, 276 eligible patients were admitted for colorectal procedures. The risk algorithm stratified 203 (73.6%) as the low-risk group and 73 (26.4%) as the high-risk group. Among the 214 (77.5%) patients with available data, high-risk patients were younger than low-risk patients (age: median 53, IQR 40-65 years, vs median 59, IQR 49-69 years, median difference five years, 95% CI 1-9; P=.02) and were more often female patients (45/73, 62% vs 80/203, 39.4%; odds ratio 2.5, 95% CI 1.4-4.5; P=.002). The risk stratification was reasonably specific (true negative rate=144/200, 72%) but not sensitive (true positive rate=10/31, 32%). Only 39.7% (85/214) patients completed any postoperative quality of recovery questionnaires (only 14, 6.5% patients beyond 60 days after surgery), and 22.9% (49/214) completed a postdischarge medication survey. Interviewed participants welcomed the initiative but noted usability issues and poor platform education.</p><p><strong>Conclusions: </strong>An initial POQI platform prototype was deployed operationally; the risk algorithm had reasonable specificity but poor sensitivity. There was a significant loss to follow-up in postdischarge survey completion. Clinicians and patients appreciated the potential impact of preemptively addressing opioid exposure but expressed shortcomings in the platform's design and implementation. Iterative platform redesign with additional features and reevaluation are required before broader implementation.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":"7 ","pages":"e54926"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11252618/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/54926","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
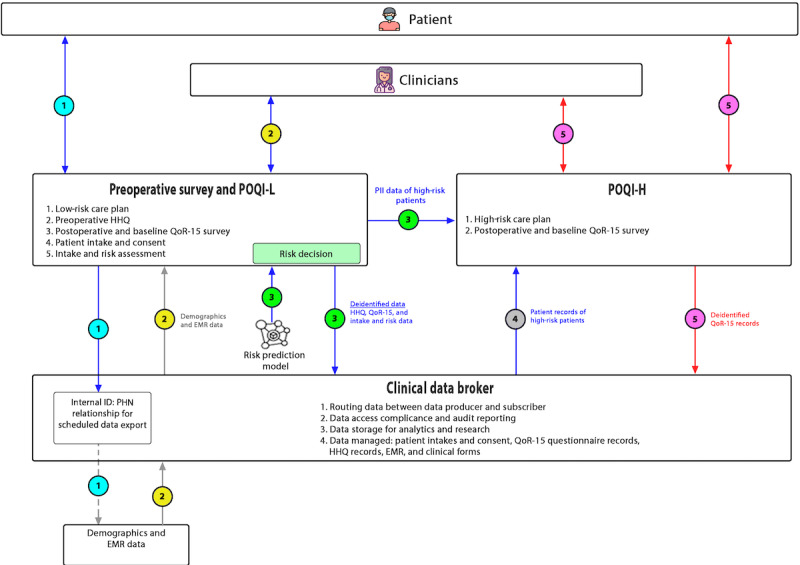
Background: Exposure to opioids after surgery is the initial contact for some people who develop chronic opioid use disorder. Hence, effective postoperative pain management, with less reliance on opioids, is critical. The Perioperative Opioid Quality Improvement (POQI) program developed (1) a digital health platform leveraging patient-survey-reported risk factors and (2) a postsurgical pain risk stratification algorithm to personalize perioperative care by integrating several commercially available digital health solutions into a combined platform. Development was reduced in scope by the COVID-19 pandemic.
Objective: This pilot study aims to assess the screening performance of the risk algorithm, quantify the use of the POQI platform, and evaluate clinicians' and patients' perceptions of its utility and benefit.
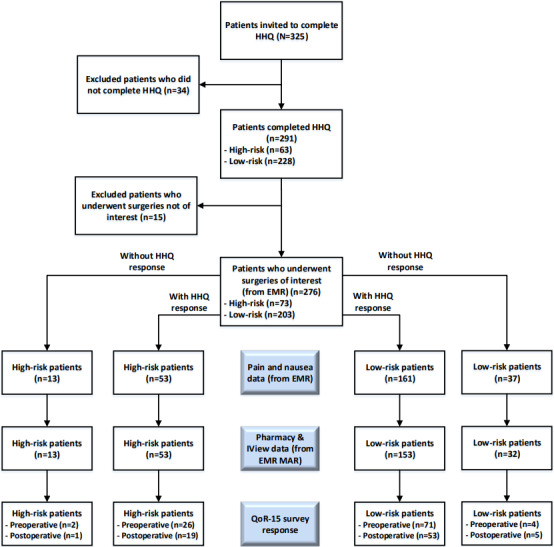
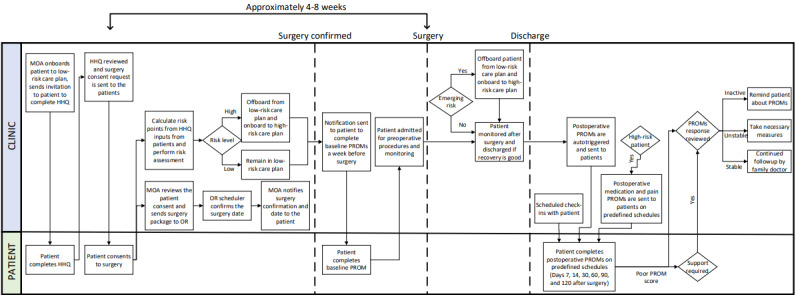
Methods: A POQI platform prototype was implemented in a quality improvement initiative at a Canadian tertiary care center and evaluated from January to September 2022. After surgical booking, a preliminary risk stratification algorithm was applied to health history questionnaire responses. The estimated risk guided the patient assignment to a care pathway based on low or high risk for persistent pain and opioid use. Demographic, procedural, and medication administration data were extracted retrospectively from the electronic medical record. Postoperative inpatient opioid use of >90 morphine milligram equivalents per day was the outcome used to assess algorithm performance. Data were summarized and compared between the low- and high-risk groups. POQI use was assessed by completed surveys on postoperative days 7, 14, 30, 60, 90, and 120. Semistructured patient and clinician interviews provided qualitative feedback on the platform.
Results: Overall, 276 eligible patients were admitted for colorectal procedures. The risk algorithm stratified 203 (73.6%) as the low-risk group and 73 (26.4%) as the high-risk group. Among the 214 (77.5%) patients with available data, high-risk patients were younger than low-risk patients (age: median 53, IQR 40-65 years, vs median 59, IQR 49-69 years, median difference five years, 95% CI 1-9; P=.02) and were more often female patients (45/73, 62% vs 80/203, 39.4%; odds ratio 2.5, 95% CI 1.4-4.5; P=.002). The risk stratification was reasonably specific (true negative rate=144/200, 72%) but not sensitive (true positive rate=10/31, 32%). Only 39.7% (85/214) patients completed any postoperative quality of recovery questionnaires (only 14, 6.5% patients beyond 60 days after surgery), and 22.9% (49/214) completed a postdischarge medication survey. Interviewed participants welcomed the initiative but noted usability issues and poor platform education.
Conclusions: An initial POQI platform prototype was deployed operationally; the risk algorithm had reasonable specificity but poor sensitivity. There was a significant loss to follow-up in postdischarge survey completion. Clinicians and patients appreciated the potential impact of preemptively addressing opioid exposure but expressed shortcomings in the platform's design and implementation. Iterative platform redesign with additional features and reevaluation are required before broader implementation.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
