{"title":"Vulvovaginal lichen planus mimicking desquamative inflammatory vulvovaginitis: A case series","authors":"Marlene Wijaya BMed, MD, MPhil, Rebecca Bronwyn Saunderson BMedSci (hon1), MBBS (hon), MPhil (Cantab), FACD, Gayle Fischer MBBS (hon1), MD, FACD","doi":"10.1111/ajd.14344","DOIUrl":null,"url":null,"abstract":"<p>Vulvovaginal lichen planus (VLP) is a chronic inflammatory dermatosis of the vulva with or without vaginal involvement. Its diagnosis can be challenging due to variations in morphology and histopathological findings. In 1988, Edwards and Friedrich reported a case series of VLP patients whose clinical presentation mimicked desquamative inflammatory vulvovaginitis (DIV).<span><sup>1</sup></span> DIV is an uncommon non-infective vulvovaginitis, characterised by pain, dyspareunia, pruritus and white or green non-offensive discharge. However, unlike VLP is not a scarring condition.<span><sup>2</sup></span> Herein we present a case series of women who were initially diagnosed with DIV but did not respond to treatment with topical clindamycin which is usually highly effective (Table 1). When their diagnosis was revised, they improved following treatment appropriate for VLP.</p><p>To our knowledge, this is the only other case series since 1988 to report patients with DIV-like VLP. DIV and VLP can pose significant diagnostic challenges as both have a wide range of clinical manifestations and histopathological findings, which often overlap. On histology, lichenoid infiltrate can be found in either condition, and the observed changes are often reported as ‘non-specific’. Additionally, the two conditions have a predilection for peri-/post-menopausal women.<span><sup>3, 4</sup></span></p><p>Desquamative inflammatory vulvovaginitis is typically characterised by vulval pain, dyspareunia and purulent white or green non-offensive discharge.<span><sup>5, 6</sup></span> Erythema and petechiae or punctate erosions are usually observed on examination.<span><sup>2, 3</sup></span> Meanwhile, in VLP, purulent discharge is not normally observed. DIV does not result in scarring, whereas VLP typically presents with glazed erythema, erosions and hyperkeratosis and frequently, if untreated causes scarring, loss of vulval structure and stenosis of the vagina.<span><sup>7</sup></span> There can also be associated oral mucosal involvement (oral lichen planus) which is not observed in DIV. In our case series, petechiae were consistently observed in all patients. This suggests that although petechiae are not common findings in VLP,<span><sup>8</sup></span> these may re-present a small sub-type of VLP mimicking DIV. Additionally, as in case 3, oral mucosal involvement may provide an additional clue pointing to a diagnosis of VLP.</p><p>Treatment resistance should also prompt clinicians to consider an alternative diagnosis, as DIV usually responds promptly to topical antibiotic treatments, particularly 2% clindamycin. A study by Bradford et al. compared 101 cases of DIV to 75 cases of VLP.<span><sup>2</sup></span> The majority of DIV patients (94%) were responsive to 4–6 weeks of intravaginal clindamycin 2%, with 35% requiring maintenance therapy. In another study by Sobel et al. of 130 DIV patients over a 12-year period, 86% of the patients reported significant symptom improvement within 3 weeks of being commenced on clindamycin 2% or hydrocortisone 10% cream.</p><p>Historical triggers have been reported as potential differentiators between DIV and VLP. In the study by Bradford et al., more than half of DIV patients (56%) reported historical triggers, compared to only 15% in the VLP group (<i>p</i> < 0.0001).<span><sup>2</sup></span> Some of the documented triggers included diarrhoea, prolonged antibiotic use and acute genital infection. In the presented case series, two patients had suspected chronic vulvovaginal candidiasis (CVVC). One patient had a drug reaction with eosinophilia and systemic symptoms (DRESS) due to lamotrigine prior to the disease onset.</p><p>It would also appear that DIV like VLP is a challenge to treat. Only one of our patients was able to achieve control with topical corticosteroids with all others requiring systemic treatments.</p><p>In summary, VLP can present with signs and symptoms mimicking DIV. In patients who have been diagnosed with DIV and demonstrate treatment resistance, an alternative diagnosis of VLP should be considered. The involvement of other body sites, such as oral mucosa, can also help in making the diagnosis of VLP. This subgroup of VLP appears to require systemic treatment in most cases.</p><p>None reported.</p><p>Ethics approval has been obtained from the Ramsay Health Care Human Research Ethics Committee.</p><p>All patients have consented to the inclusion of their cases in this report for journal publication. Consent has been obtained from patients, whose photos are included in this report.</p>","PeriodicalId":8638,"journal":{"name":"Australasian Journal of Dermatology","volume":"65 7","pages":"e203-e207"},"PeriodicalIF":1.8000,"publicationDate":"2024-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ajd.14344","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Australasian Journal of Dermatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ajd.14344","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Vulvovaginal lichen planus (VLP) is a chronic inflammatory dermatosis of the vulva with or without vaginal involvement. Its diagnosis can be challenging due to variations in morphology and histopathological findings. In 1988, Edwards and Friedrich reported a case series of VLP patients whose clinical presentation mimicked desquamative inflammatory vulvovaginitis (DIV).1 DIV is an uncommon non-infective vulvovaginitis, characterised by pain, dyspareunia, pruritus and white or green non-offensive discharge. However, unlike VLP is not a scarring condition.2 Herein we present a case series of women who were initially diagnosed with DIV but did not respond to treatment with topical clindamycin which is usually highly effective (Table 1). When their diagnosis was revised, they improved following treatment appropriate for VLP.
To our knowledge, this is the only other case series since 1988 to report patients with DIV-like VLP. DIV and VLP can pose significant diagnostic challenges as both have a wide range of clinical manifestations and histopathological findings, which often overlap. On histology, lichenoid infiltrate can be found in either condition, and the observed changes are often reported as ‘non-specific’. Additionally, the two conditions have a predilection for peri-/post-menopausal women.3, 4
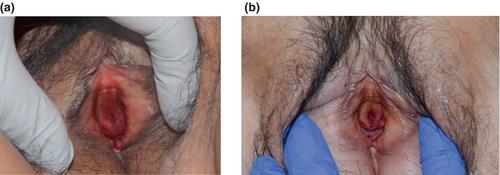
Desquamative inflammatory vulvovaginitis is typically characterised by vulval pain, dyspareunia and purulent white or green non-offensive discharge.5, 6 Erythema and petechiae or punctate erosions are usually observed on examination.2, 3 Meanwhile, in VLP, purulent discharge is not normally observed. DIV does not result in scarring, whereas VLP typically presents with glazed erythema, erosions and hyperkeratosis and frequently, if untreated causes scarring, loss of vulval structure and stenosis of the vagina.7 There can also be associated oral mucosal involvement (oral lichen planus) which is not observed in DIV. In our case series, petechiae were consistently observed in all patients. This suggests that although petechiae are not common findings in VLP,8 these may re-present a small sub-type of VLP mimicking DIV. Additionally, as in case 3, oral mucosal involvement may provide an additional clue pointing to a diagnosis of VLP.
Treatment resistance should also prompt clinicians to consider an alternative diagnosis, as DIV usually responds promptly to topical antibiotic treatments, particularly 2% clindamycin. A study by Bradford et al. compared 101 cases of DIV to 75 cases of VLP.2 The majority of DIV patients (94%) were responsive to 4–6 weeks of intravaginal clindamycin 2%, with 35% requiring maintenance therapy. In another study by Sobel et al. of 130 DIV patients over a 12-year period, 86% of the patients reported significant symptom improvement within 3 weeks of being commenced on clindamycin 2% or hydrocortisone 10% cream.
Historical triggers have been reported as potential differentiators between DIV and VLP. In the study by Bradford et al., more than half of DIV patients (56%) reported historical triggers, compared to only 15% in the VLP group (p < 0.0001).2 Some of the documented triggers included diarrhoea, prolonged antibiotic use and acute genital infection. In the presented case series, two patients had suspected chronic vulvovaginal candidiasis (CVVC). One patient had a drug reaction with eosinophilia and systemic symptoms (DRESS) due to lamotrigine prior to the disease onset.
It would also appear that DIV like VLP is a challenge to treat. Only one of our patients was able to achieve control with topical corticosteroids with all others requiring systemic treatments.
In summary, VLP can present with signs and symptoms mimicking DIV. In patients who have been diagnosed with DIV and demonstrate treatment resistance, an alternative diagnosis of VLP should be considered. The involvement of other body sites, such as oral mucosa, can also help in making the diagnosis of VLP. This subgroup of VLP appears to require systemic treatment in most cases.
None reported.
Ethics approval has been obtained from the Ramsay Health Care Human Research Ethics Committee.
All patients have consented to the inclusion of their cases in this report for journal publication. Consent has been obtained from patients, whose photos are included in this report.
期刊介绍:
Australasian Journal of Dermatology is the official journal of the Australasian College of Dermatologists and the New Zealand Dermatological Society, publishing peer-reviewed, original research articles, reviews and case reports dealing with all aspects of clinical practice and research in dermatology. Clinical presentations, medical and physical therapies and investigations, including dermatopathology and mycology, are covered. Short articles may be published under the headings ‘Signs, Syndromes and Diagnoses’, ‘Dermatopathology Presentation’, ‘Vignettes in Contact Dermatology’, ‘Surgery Corner’ or ‘Letters to the Editor’.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
