Tara Reshadmanesh, Amir Hossein Behnoush, Maedeh Farajollahi, Amirmohammad Khalaji, Elina Ghondaghsaz, Hassan Ahangar
{"title":"Circulating Levels of Calprotectin as a Biomarker in Patients With Coronary Artery Disease: A Systematic Review and Meta-Analysis","authors":"Tara Reshadmanesh, Amir Hossein Behnoush, Maedeh Farajollahi, Amirmohammad Khalaji, Elina Ghondaghsaz, Hassan Ahangar","doi":"10.1002/clc.24315","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Calprotectin, also known as MRP8/14, is generated by immune cells and is altered in several inflammatory diseases. Studies have assessed their levels in patients with coronary artery disease (CAD) and its subtypes (stable CAD and acute coronary syndrome [ACS]). Herein, we aimed to systematically investigate these associations through a systematic review and meta-analysis.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A systematic search was conducted in four online databases, including PubMed, Scopus, Embase, and the Web of Science. Relevant studies were retrieved, screened, and extracted. Random-effect meta-analysis was performed for the calculation of standardized mean difference (SMD) and 95% confidence interval (CI). Blood calprotectin levels were compared between CAD patients and controls, as well as CAD subtypes.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 20 studies were included in the systematic review and meta-analysis, comprising 3300 CAD patients and 1230 controls. Patients with CAD had significantly higher calprotectin levels (SMD 0.81, 95% CI 0.32−1.30, <i>p</i> < 0.01). Similarly, patients with ACS were reported to have higher levels compared to those with stable CAD. However, there was no significant difference in terms of blood calprotectin levels between stable CAD cases and healthy controls. Finally, studies have shown that calprotectin could be used as a diagnostic biomarker of CAD while also predicting major adverse events and mortality in these patients.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Based on our findings, calprotectin, as an inflammatory marker, could be used as a possible biomarker for patients with CAD and ACS. These suggest the possibility of pathophysiological pathways for this involvement and warrant further research on these associations as well as their clinical utility.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 7","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24315","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.24315","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Calprotectin, also known as MRP8/14, is generated by immune cells and is altered in several inflammatory diseases. Studies have assessed their levels in patients with coronary artery disease (CAD) and its subtypes (stable CAD and acute coronary syndrome [ACS]). Herein, we aimed to systematically investigate these associations through a systematic review and meta-analysis.
Methods
A systematic search was conducted in four online databases, including PubMed, Scopus, Embase, and the Web of Science. Relevant studies were retrieved, screened, and extracted. Random-effect meta-analysis was performed for the calculation of standardized mean difference (SMD) and 95% confidence interval (CI). Blood calprotectin levels were compared between CAD patients and controls, as well as CAD subtypes.
Results
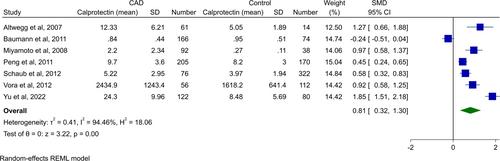
A total of 20 studies were included in the systematic review and meta-analysis, comprising 3300 CAD patients and 1230 controls. Patients with CAD had significantly higher calprotectin levels (SMD 0.81, 95% CI 0.32−1.30, p < 0.01). Similarly, patients with ACS were reported to have higher levels compared to those with stable CAD. However, there was no significant difference in terms of blood calprotectin levels between stable CAD cases and healthy controls. Finally, studies have shown that calprotectin could be used as a diagnostic biomarker of CAD while also predicting major adverse events and mortality in these patients.
Conclusion
Based on our findings, calprotectin, as an inflammatory marker, could be used as a possible biomarker for patients with CAD and ACS. These suggest the possibility of pathophysiological pathways for this involvement and warrant further research on these associations as well as their clinical utility.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
