Raanan Meyer, Kacey M. Hamilton, Rebecca J. Schneyer, Gabriel Levin, Mireille D. Truong, Matthew T. Siedhoff, Kelly N. Wright
{"title":"Costs and carbon emissions of virtual preoperative visits implementation","authors":"Raanan Meyer, Kacey M. Hamilton, Rebecca J. Schneyer, Gabriel Levin, Mireille D. Truong, Matthew T. Siedhoff, Kelly N. Wright","doi":"10.1111/1471-0528.17906","DOIUrl":null,"url":null,"abstract":"<p>The rise in carbon dioxide (CO<sub>2</sub>) in the atmosphere has contributed significantly to climate change, which has been called the greatest threat to human health.<span><sup>1, 2</sup></span> The healthcare system accounts for 4.4% of all CO<sub>2</sub> emissions worldwide, more than global aviation, with the United States contributing 27% of this effect.<span><sup>3, 4</sup></span> Telemedicine has been adopted in various medical disciplines with the emergence of the SARS-CoV2 pandemic and has been shown to reduce costs.<span><sup>1, 5</sup></span> Currently, data regarding the sustainability effect of preoperative visits in gynaecology are limited. We aimed to evaluate the economic and carbon emission effects of preoperative visit types, virtual versus in-person in the office, in a minimally invasive gynaecologic surgery practice.</p><p>All women who underwent surgery with a Division of Minimally Invasive Gynecologic Surgery at a high-volume urban referral quaternary care centre from January 2016 to May 2023 were included. The Division of Minimally Invasive Gynecologic Surgery treats benign gynaecologic conditions only. Virtual consultations, preoperative and postoperative visits were implemented in March 2020, during the COVID-19 pandemic, and have continued to the present day. Prior to March 2020, all patients were seen in person, at our outpatient clinic. After March 2020, decision on the type of preoperative visit since the pandemic was according to clinic closures due to infection surges, patients' preferences and providers' permission, though most patients were recommended to be seen virtually for their initial consultation if an in-office procedure was not required. Patients who experienced both types of visits prior to surgery, virtual and in-person, were excluded. We analysed the costs associated with driving to office visits, driving times, distances and costs, CO<sub>2</sub> emissions, as well as patient characteristics, surgical characteristics and complications defined according to the Clavien–Dindo classification. Driving distances, times and CO<sub>2</sub> emissions were calculated based on patients' zip codes and their distance to the office (Data S1). Virtual and office visits were compared. The primary outcome was the quantification in driving costs, driving times and CO<sub>2</sub> emissions for each group.</p><p>A total of 1196 and 1751 women had preoperative virtual and office visits, respectively (Tables 1 and S1). Median age was lower in the group of virtual visits (37.0 vs. 40.0 years, <i>p</i> < 0.001). There was a higher proportion of stage IV endometriosis (16.4% vs. 7.8%, <i>p</i> < 0.001) and minimally invasive surgery (89.7% vs 77.7%, <i>p</i> < 0.001) in the virtual group compared to the office visit group. Complication proportions were similar in both groups (5.9% virtual vs. 6.3% office groups, <i>p</i> = 0.639, Table S2). Intraoperative complication proportion was significantly lower in the virtual visits' groups, but comparable after multivariable regression analysis (<i>p</i> = 0.262). Any complications remained comparable between groups after multivariable regression analysis (<i>p</i> = 0.733). The 1751 preoperative office visits resulted in a total of $29 381.78 driving costs, 22 899.61 kg of CO<sub>2</sub> emission, 55 716.82 driving miles and 104 429.64 driving minutes/1740.49 h (Figure 1). Per patient, median driving cost was $16.78, CO<sub>2</sub> emission was 13.08 kg, driving distance was 31.82 miles and driving time was 59.64 min. Those who had a preoperative virtual visit had more preoperative visits (median 1.00 for both groups, <i>p</i> < 0.001) and less postoperative visits (median 1.00 for both groups, <i>p</i> < 0.001) than women who had a preoperative office visit. The total postoperative office driving costs, CO<sub>2</sub> emissions, driving distance and driving times were 11.3 times lower for the patients who had preoperative virtual visits and postoperative office visits (111/1196, 9.3%) than for the patients who had preoperative and postoperative office visits (1254/1751, 71.6%).</p><p>Preoperative virtual visits resulted in significantly reduced driving costs, CO<sub>2</sub> emissions and driving time compared to preoperative office visits, without impacting intraoperative and postoperative outcomes. The prevented carbon emission load for the virtual visit group is equivalent to the amount of carbon sequestered, for example, by 18.7 acres of forest in 1 year, or emitted by driving more than 40 K miles in an average car.<span><sup>6</sup></span> Time saved by patients in the virtual visits extends beyond driving time only, as it may include time off work and parking time, two parameters that were not included in the analysis.<span><sup>1</sup></span> Limitations of this study include its retrospective design, single-centre setting, inclusion of patients of relatively high socioeconomic status and calculation based on zip codes that may not be accurate.<span><sup>7</sup></span></p><p>RM- conception, design, acquisition of data, analysis and interpretation of data, drafting the article, approval of the final version; KH- acquisition of data, critical revision of the article, approval of the final version; RS- acquisition of data, critical revision of the article, approval of the final version; GL- conception and design, analysis and interpretation of data, critical revision of the article, approval of the final version; MT- acquisition of data, critical revision of the article, approval of the final version; MS- acquisition of data, critical revision of the article, approval of the final version; KW- conception, design, acquisition of data, critical revision of the article, approval of the final version.</p><p>No funding was received for this research.</p><p>MT- consultant for Ethicon, Medtronic, Heracure Medical and Cooper Surgical; MS- consultant for Applied Medical and Intuitive Surgical; KW- consultant for Aqua Therapeutics, Hologic, Ethicon and Karl Storz; RM- consultant for Intuitive Surgical. All other authors report no conflicts of interest.</p><p>The study received approval from the institutional review board at Cedars-Sinai Medical Center (#00001714, 8/28/2023).</p><p>Cedars Sinai Medical Center, Los Angeles, CA, USA.</p>","PeriodicalId":50729,"journal":{"name":"Bjog-An International Journal of Obstetrics and Gynaecology","volume":"131 13","pages":"1894-1897"},"PeriodicalIF":4.3000,"publicationDate":"2024-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1471-0528.17906","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bjog-An International Journal of Obstetrics and Gynaecology","FirstCategoryId":"3","ListUrlMain":"https://obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.17906","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
The rise in carbon dioxide (CO2) in the atmosphere has contributed significantly to climate change, which has been called the greatest threat to human health.1, 2 The healthcare system accounts for 4.4% of all CO2 emissions worldwide, more than global aviation, with the United States contributing 27% of this effect.3, 4 Telemedicine has been adopted in various medical disciplines with the emergence of the SARS-CoV2 pandemic and has been shown to reduce costs.1, 5 Currently, data regarding the sustainability effect of preoperative visits in gynaecology are limited. We aimed to evaluate the economic and carbon emission effects of preoperative visit types, virtual versus in-person in the office, in a minimally invasive gynaecologic surgery practice.
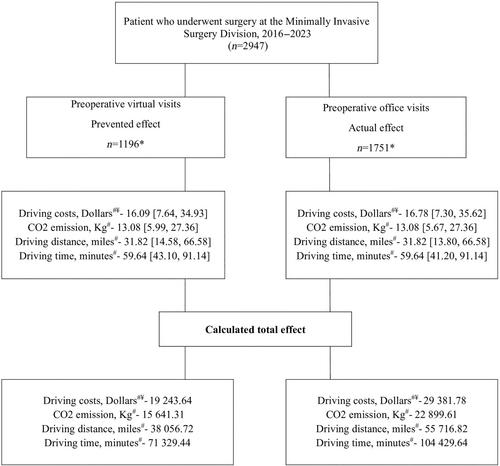
All women who underwent surgery with a Division of Minimally Invasive Gynecologic Surgery at a high-volume urban referral quaternary care centre from January 2016 to May 2023 were included. The Division of Minimally Invasive Gynecologic Surgery treats benign gynaecologic conditions only. Virtual consultations, preoperative and postoperative visits were implemented in March 2020, during the COVID-19 pandemic, and have continued to the present day. Prior to March 2020, all patients were seen in person, at our outpatient clinic. After March 2020, decision on the type of preoperative visit since the pandemic was according to clinic closures due to infection surges, patients' preferences and providers' permission, though most patients were recommended to be seen virtually for their initial consultation if an in-office procedure was not required. Patients who experienced both types of visits prior to surgery, virtual and in-person, were excluded. We analysed the costs associated with driving to office visits, driving times, distances and costs, CO2 emissions, as well as patient characteristics, surgical characteristics and complications defined according to the Clavien–Dindo classification. Driving distances, times and CO2 emissions were calculated based on patients' zip codes and their distance to the office (Data S1). Virtual and office visits were compared. The primary outcome was the quantification in driving costs, driving times and CO2 emissions for each group.
A total of 1196 and 1751 women had preoperative virtual and office visits, respectively (Tables 1 and S1). Median age was lower in the group of virtual visits (37.0 vs. 40.0 years, p < 0.001). There was a higher proportion of stage IV endometriosis (16.4% vs. 7.8%, p < 0.001) and minimally invasive surgery (89.7% vs 77.7%, p < 0.001) in the virtual group compared to the office visit group. Complication proportions were similar in both groups (5.9% virtual vs. 6.3% office groups, p = 0.639, Table S2). Intraoperative complication proportion was significantly lower in the virtual visits' groups, but comparable after multivariable regression analysis (p = 0.262). Any complications remained comparable between groups after multivariable regression analysis (p = 0.733). The 1751 preoperative office visits resulted in a total of $29 381.78 driving costs, 22 899.61 kg of CO2 emission, 55 716.82 driving miles and 104 429.64 driving minutes/1740.49 h (Figure 1). Per patient, median driving cost was $16.78, CO2 emission was 13.08 kg, driving distance was 31.82 miles and driving time was 59.64 min. Those who had a preoperative virtual visit had more preoperative visits (median 1.00 for both groups, p < 0.001) and less postoperative visits (median 1.00 for both groups, p < 0.001) than women who had a preoperative office visit. The total postoperative office driving costs, CO2 emissions, driving distance and driving times were 11.3 times lower for the patients who had preoperative virtual visits and postoperative office visits (111/1196, 9.3%) than for the patients who had preoperative and postoperative office visits (1254/1751, 71.6%).
Preoperative virtual visits resulted in significantly reduced driving costs, CO2 emissions and driving time compared to preoperative office visits, without impacting intraoperative and postoperative outcomes. The prevented carbon emission load for the virtual visit group is equivalent to the amount of carbon sequestered, for example, by 18.7 acres of forest in 1 year, or emitted by driving more than 40 K miles in an average car.6 Time saved by patients in the virtual visits extends beyond driving time only, as it may include time off work and parking time, two parameters that were not included in the analysis.1 Limitations of this study include its retrospective design, single-centre setting, inclusion of patients of relatively high socioeconomic status and calculation based on zip codes that may not be accurate.7
RM- conception, design, acquisition of data, analysis and interpretation of data, drafting the article, approval of the final version; KH- acquisition of data, critical revision of the article, approval of the final version; RS- acquisition of data, critical revision of the article, approval of the final version; GL- conception and design, analysis and interpretation of data, critical revision of the article, approval of the final version; MT- acquisition of data, critical revision of the article, approval of the final version; MS- acquisition of data, critical revision of the article, approval of the final version; KW- conception, design, acquisition of data, critical revision of the article, approval of the final version.
No funding was received for this research.
MT- consultant for Ethicon, Medtronic, Heracure Medical and Cooper Surgical; MS- consultant for Applied Medical and Intuitive Surgical; KW- consultant for Aqua Therapeutics, Hologic, Ethicon and Karl Storz; RM- consultant for Intuitive Surgical. All other authors report no conflicts of interest.
The study received approval from the institutional review board at Cedars-Sinai Medical Center (#00001714, 8/28/2023).
Cedars Sinai Medical Center, Los Angeles, CA, USA.
7RM-构思、设计、获取数据、分析和解释数据、起草文章、批准最终版本;KH-获取数据、严格修改文章、批准最终版本;RS-获取数据、严格修改文章、批准最终版本;GL-构思和设计、分析和解释数据、对文章进行重要修改、批准最终版本;MT-获取数据、对文章进行重要修改、批准最终版本;MS-获取数据、对文章进行重要修改、批准最终版本;KW-构思、设计、获取数据、对文章进行重要修改、批准最终版本。MT- Ethicon、Medtronic、Heracure Medical 和 Cooper Surgical 的顾问;MS- Applied Medical 和 Intuitive Surgical 的顾问;KW- Aqua Therapeutics、Hologic、Ethicon 和 Karl Storz 的顾问;RM- Intuitive Surgical 的顾问。所有其他作者均未报告利益冲突。该研究获得了雪松西奈医疗中心机构审查委员会的批准(#00001714, 8/28/2023)。
期刊介绍:
BJOG is an editorially independent publication owned by the Royal College of Obstetricians and Gynaecologists (RCOG). The Journal publishes original, peer-reviewed work in all areas of obstetrics and gynaecology, including contraception, urogynaecology, fertility, oncology and clinical practice. Its aim is to publish the highest quality medical research in women''s health, worldwide.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
