{"title":"Effective use of the two-devices-in-one-channel technique for stent exchange following endoscopic ultrasound-guided hepaticogastrostomy","authors":"Yasuhiro Kuraishi, Ichitaro Horiuchi, Akira Nakamura","doi":"10.1111/den.14875","DOIUrl":null,"url":null,"abstract":"<p>Plastic stent (PS) exchange after endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) is considered a routine procedure. However, when biliary access through the existing fistula is lost, additional fistuloplasty is required to restore drainage. Guidewire insertion alongside the existing PS before removal is therefore recommended to maintain access and prevent this complication.<span><sup>1</sup></span> The two-devices-in-one-channel technique is effective for trans-papillary biliary cannulation, particularly in cases involving juxtapapillary diverticulum.<span><sup>2, 3</sup></span> We recently employed this approach in a challenging case of PS exchange post-EUS-HGS.</p><p>A 70-year-old man suffered acute cholangitis from choledochojejunal anastomotic stricture after extended cholecystectomy. Initial biliary drainage using balloon-assisted endoscopy failed because the scope could not reach the anastomosis, and percutaneous trans-hepatic biliary drainage (PTBD) was subsequently performed. To internalize biliary drainage, EUS-HGS was conducted by placing a 7F PS (ThroughPass TYPE IT; Gadelius Medical, Tokyo, Japan) into the left intrahepatic bile duct to remove the PTBD tube (Fig. 1). During the scheduled PS exchange using a duodenoscope (TJF-Q290V; Olympus, Tokyo, Japan), however, guidewire insertion into the bile duct alongside the stent proved challenging. The scope's position was distant from the fistula despite various manipulations, including air aspiration, and the steep downward angle of the PS further complicated guidewire insertion. We employed the two-devices-in-one-channel technique, inserting a tapered catheter (PR-110Q-1; Olympus) loaded with a 0.025 inch guidewire along with small biopsy forceps (FB45Q-1; Olympus) into the same scope channel (Fig. 2). The forceps grasped the proximal PS flange and pulled it towards the scope, allowing the scope to be positioned closer to the fistula and aligning the fistula axis with the catheter. This approach enabled successful guidewire insertion into the bile duct alongside the stent. After removing the existing PS and balloon dilating the anastomosis, a new PS was successfully placed (Video S1). The two-devices-in-one-channel technique demonstrated effectiveness in overcoming a significant challenge associated with PS exchange post-EUS-HGS.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 9","pages":"1056-1058"},"PeriodicalIF":4.7000,"publicationDate":"2024-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14875","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14875","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Plastic stent (PS) exchange after endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) is considered a routine procedure. However, when biliary access through the existing fistula is lost, additional fistuloplasty is required to restore drainage. Guidewire insertion alongside the existing PS before removal is therefore recommended to maintain access and prevent this complication.1 The two-devices-in-one-channel technique is effective for trans-papillary biliary cannulation, particularly in cases involving juxtapapillary diverticulum.2, 3 We recently employed this approach in a challenging case of PS exchange post-EUS-HGS.
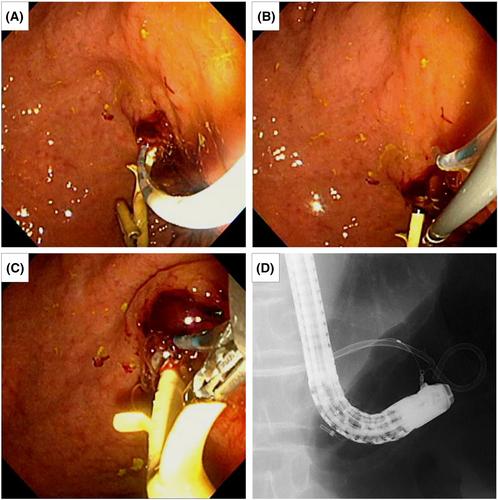
A 70-year-old man suffered acute cholangitis from choledochojejunal anastomotic stricture after extended cholecystectomy. Initial biliary drainage using balloon-assisted endoscopy failed because the scope could not reach the anastomosis, and percutaneous trans-hepatic biliary drainage (PTBD) was subsequently performed. To internalize biliary drainage, EUS-HGS was conducted by placing a 7F PS (ThroughPass TYPE IT; Gadelius Medical, Tokyo, Japan) into the left intrahepatic bile duct to remove the PTBD tube (Fig. 1). During the scheduled PS exchange using a duodenoscope (TJF-Q290V; Olympus, Tokyo, Japan), however, guidewire insertion into the bile duct alongside the stent proved challenging. The scope's position was distant from the fistula despite various manipulations, including air aspiration, and the steep downward angle of the PS further complicated guidewire insertion. We employed the two-devices-in-one-channel technique, inserting a tapered catheter (PR-110Q-1; Olympus) loaded with a 0.025 inch guidewire along with small biopsy forceps (FB45Q-1; Olympus) into the same scope channel (Fig. 2). The forceps grasped the proximal PS flange and pulled it towards the scope, allowing the scope to be positioned closer to the fistula and aligning the fistula axis with the catheter. This approach enabled successful guidewire insertion into the bile duct alongside the stent. After removing the existing PS and balloon dilating the anastomosis, a new PS was successfully placed (Video S1). The two-devices-in-one-channel technique demonstrated effectiveness in overcoming a significant challenge associated with PS exchange post-EUS-HGS.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
