{"title":"Caesarean section and anal incontinence in women after obstetric anal sphincter injury: A systematic review and meta-analysis","authors":"Emily Carter, Rebecca Hall, Kelechi Ajoku, Jenny Myers, Rohna Kearney","doi":"10.1111/1471-0528.17899","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Approximately 50% women who give birth after obstetric anal sphincter injury (OASI) develop anal incontinence (AI) over their lifetime.</p>\n </section>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>To evaluate current evidence for a protective benefit of planned caesarean section (CS) to prevent AI after OASI.</p>\n </section>\n \n <section>\n \n <h3> Search Strategy</h3>\n \n <p>MEDLINE/PubMed, Embase 1974–2024, CINAHL and Cochrane to 7 February 2024 (PROSPERO CRD42022372442).</p>\n </section>\n \n <section>\n \n <h3> Selection Criteria</h3>\n \n <p>All studies reporting outcomes after OASI and a subsequent birth, by any mode.</p>\n </section>\n \n <section>\n \n <h3> Data Collection and Analysis</h3>\n \n <p>Eighty-six of 2646 screened studies met inclusion criteria, with nine studies suitable to meta-analyse the primary outcome of ‘adjusted AI’ after OASI and subsequent birth. Subgroups: short-term AI, long-term AI, AI in asymptomatic women. Secondary outcomes: total AI, quality of life, satisfaction/regret, solid/liquid/flatal incontinence, faecal urgency, AI in women with and without subsequent birth, change in AI pre- to post- subsequent birth.</p>\n </section>\n \n <section>\n \n <h3> Main Results</h3>\n \n <p>There was no evidence of a difference in adjusted AI after subsequent vaginal birth compared with CS after OASI across all time periods (OR = 0.92, 95% CI 0.72–1.20; 9 studies, 2104 participants, <i>I</i><sup>2</sup> = 0% <i>p</i> = 0.58), for subgroup analyses or secondary outcomes. There was no evidence of a difference in AI in women with or without subsequent birth (OR = 1.00 95% CI 0.65–1.54; 10 studies, 970 participants, <i>I</i><sup>2</sup> = 35% <i>p</i> = 0.99), or pre- to post- subsequent birth (OR = 0.79 95% CI 0.51–1.25; 13 studies, 5496 participants, <i>I</i><sup>2</sup> = 73% <i>p</i> = 0.31).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Due to low evidence quality, we are unable to determine whether planned caesarean is protective against AI after OASI. Higher quality evidence is required to guide personalised decision-making for asymptomatic women and to determine the effect of subsequent birth mode on long-term AI outcomes.</p>\n </section>\n </div>","PeriodicalId":50729,"journal":{"name":"Bjog-An International Journal of Obstetrics and Gynaecology","volume":"132 8","pages":"1032-1044"},"PeriodicalIF":4.3000,"publicationDate":"2024-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1471-0528.17899","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bjog-An International Journal of Obstetrics and Gynaecology","FirstCategoryId":"3","ListUrlMain":"https://obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.17899","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Approximately 50% women who give birth after obstetric anal sphincter injury (OASI) develop anal incontinence (AI) over their lifetime.
Objective
To evaluate current evidence for a protective benefit of planned caesarean section (CS) to prevent AI after OASI.
Search Strategy
MEDLINE/PubMed, Embase 1974–2024, CINAHL and Cochrane to 7 February 2024 (PROSPERO CRD42022372442).
Selection Criteria
All studies reporting outcomes after OASI and a subsequent birth, by any mode.
Data Collection and Analysis
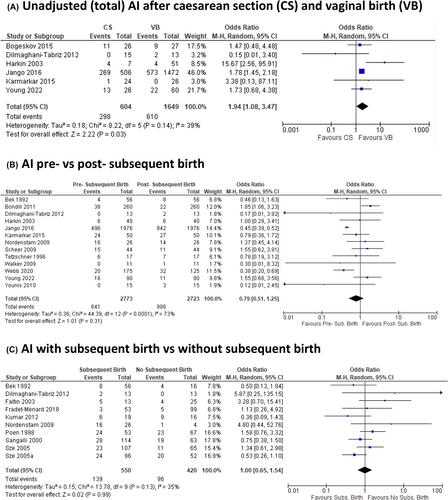
Eighty-six of 2646 screened studies met inclusion criteria, with nine studies suitable to meta-analyse the primary outcome of ‘adjusted AI’ after OASI and subsequent birth. Subgroups: short-term AI, long-term AI, AI in asymptomatic women. Secondary outcomes: total AI, quality of life, satisfaction/regret, solid/liquid/flatal incontinence, faecal urgency, AI in women with and without subsequent birth, change in AI pre- to post- subsequent birth.
Main Results
There was no evidence of a difference in adjusted AI after subsequent vaginal birth compared with CS after OASI across all time periods (OR = 0.92, 95% CI 0.72–1.20; 9 studies, 2104 participants, I2 = 0% p = 0.58), for subgroup analyses or secondary outcomes. There was no evidence of a difference in AI in women with or without subsequent birth (OR = 1.00 95% CI 0.65–1.54; 10 studies, 970 participants, I2 = 35% p = 0.99), or pre- to post- subsequent birth (OR = 0.79 95% CI 0.51–1.25; 13 studies, 5496 participants, I2 = 73% p = 0.31).
Conclusions
Due to low evidence quality, we are unable to determine whether planned caesarean is protective against AI after OASI. Higher quality evidence is required to guide personalised decision-making for asymptomatic women and to determine the effect of subsequent birth mode on long-term AI outcomes.
期刊介绍:
BJOG is an editorially independent publication owned by the Royal College of Obstetricians and Gynaecologists (RCOG). The Journal publishes original, peer-reviewed work in all areas of obstetrics and gynaecology, including contraception, urogynaecology, fertility, oncology and clinical practice. Its aim is to publish the highest quality medical research in women''s health, worldwide.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
