{"title":"Census-Dependent Mortality of Ventilated Patients With COVID-19 in Israel: Noninterventional Observational Cohort Study.","authors":"Joseph Mendlovic, Francis B Mimouni","doi":"10.2196/41749","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The COVID-19 pandemic led to several surges in the mass hospitalization rate. Extreme increases in hospital admissions without adequate medical resources may increase mortality. No study has addressed the impact of daily census of ventilated patients on mortality in the context of the pandemic in a nationwide setting.</p><p><strong>Objective: </strong>This study aimed to determine whether daily census of ventilated patients affected COVID-19 mortality rates nationwide in Israel.</p><p><strong>Methods: </strong>We conducted a cohort study using nationwide, public-domain, population-based COVID-19 data of hospitalized patients from an Israeli database from March 11, 2020, until February 11, 2021. We included all COVID-19 hospital admissions, classified as mild to severe per the Centers for Diseases Control and Prevention classification irrespective of whether they were mechanically ventilated. Outcome measures were daily death rates and death rates expressed as a percentage of ventilated patients.</p><p><strong>Results: </strong>During the study period (338 days from March 11, 2020, to February 11, 2021), 715,743 patients contracted and were clinically confirmed as having COVID-19. Among them, 5577 (0.78%) patients died. In total, 3398 patients were ventilated because of severe COVID-19. Daily mortality correlated with daily census of ventilated patients (R<sup>2</sup>=0.828, P<.001). The daily percent mortality of ventilated patients also correlated with the daily census of ventilated patients (R<sup>2</sup>=0.365, P<.001)-backward multiple regression analysis demonstrated that this positive correlation was still highly significant even when correcting for the average age or gender of ventilated patients (R<sup>2</sup>=0.4328, P<.001) or for the surge in their number. Overall, 40% of the variation in mortality was explained by variations in the daily census of ventilated patients. ANOVA revealed that at less than 50 ventilated patients per day, the daily mortality of ventilated patients was slightly above 5%, and it nearly doubled (10%) with 50-149 patients; moreover, in all categories of ≥200 patients ventilated per day, it more than tripled at ≥15% (P<.001).</p><p><strong>Conclusions: </strong>Daily mortality rates per ventilated patient increased with an increase in the number of ventilated patients, suggesting the saturation of medical resources. Policy makers should be aware that expanding medical services without adequate resources may increase mortality. Governments should perform similar analyses to provide indicators of system saturation, although further validation of these results might be needed to use this indicator to drive public policy.</p>","PeriodicalId":51757,"journal":{"name":"Interactive Journal of Medical Research","volume":"13 ","pages":"e41749"},"PeriodicalIF":1.9000,"publicationDate":"2024-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11267089/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive Journal of Medical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/41749","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The COVID-19 pandemic led to several surges in the mass hospitalization rate. Extreme increases in hospital admissions without adequate medical resources may increase mortality. No study has addressed the impact of daily census of ventilated patients on mortality in the context of the pandemic in a nationwide setting.
Objective: This study aimed to determine whether daily census of ventilated patients affected COVID-19 mortality rates nationwide in Israel.
Methods: We conducted a cohort study using nationwide, public-domain, population-based COVID-19 data of hospitalized patients from an Israeli database from March 11, 2020, until February 11, 2021. We included all COVID-19 hospital admissions, classified as mild to severe per the Centers for Diseases Control and Prevention classification irrespective of whether they were mechanically ventilated. Outcome measures were daily death rates and death rates expressed as a percentage of ventilated patients.
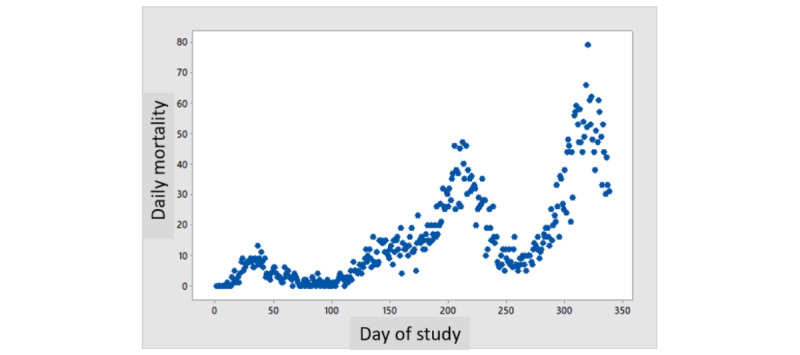
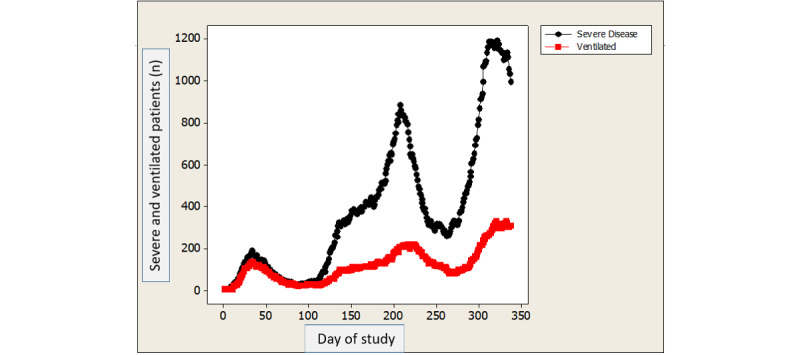
Results: During the study period (338 days from March 11, 2020, to February 11, 2021), 715,743 patients contracted and were clinically confirmed as having COVID-19. Among them, 5577 (0.78%) patients died. In total, 3398 patients were ventilated because of severe COVID-19. Daily mortality correlated with daily census of ventilated patients (R2=0.828, P<.001). The daily percent mortality of ventilated patients also correlated with the daily census of ventilated patients (R2=0.365, P<.001)-backward multiple regression analysis demonstrated that this positive correlation was still highly significant even when correcting for the average age or gender of ventilated patients (R2=0.4328, P<.001) or for the surge in their number. Overall, 40% of the variation in mortality was explained by variations in the daily census of ventilated patients. ANOVA revealed that at less than 50 ventilated patients per day, the daily mortality of ventilated patients was slightly above 5%, and it nearly doubled (10%) with 50-149 patients; moreover, in all categories of ≥200 patients ventilated per day, it more than tripled at ≥15% (P<.001).
Conclusions: Daily mortality rates per ventilated patient increased with an increase in the number of ventilated patients, suggesting the saturation of medical resources. Policy makers should be aware that expanding medical services without adequate resources may increase mortality. Governments should perform similar analyses to provide indicators of system saturation, although further validation of these results might be needed to use this indicator to drive public policy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
