{"title":"Beyond flashing lights and sirens: Community paramedicine as health safety nets for older adults","authors":"Alexander J. Ulintz MD, Carmen E. Quatman MD, PhD","doi":"10.1111/jgs.19087","DOIUrl":null,"url":null,"abstract":"<p>Providing unscheduled, acute, and longitudinal care to older adults who are aging in place is a critical, yet largely unsolved, health system challenge. A large gap exists between the times and places where older adults need care and the resources available to address those needs.<span><sup>1</sup></span> Despite efforts to increase older adults' access to in-home care through home-based primary care, telemedicine, and workforce development, persistent gaps prompted recent calls by the American Geriatrics Society and the American Association of Geriatric Psychiatry to expand the “team based geriatric physician and health professional workforce by nontraditional means.”<span><sup>2, 3</sup></span> This creates an opportunity for innovative, multidisciplinary, patient-centered teams to bridge the gap.</p><p>Emergency medical services (EMS) agencies and clinicians are often called upon to fill this gap: they are accessible, mobile, and a trusted source of care in communities across the nation.<span><sup>4</sup></span> Though originally designed for emergency treatment and transportation of the critically ill and injured, EMS clinicians are increasingly embracing roles that span community outreach, prevention, and chronic disease management in a model of care known as “community paramedicine.”<span><sup>5</sup></span> Community paramedicine is designed to fill the space between fixed medical system resources and dynamic community needs by leveraging availability, accessibility, and versatile skills of EMS clinicians working as part of physician-led or multidisciplinary team. This model of care is of clear importance to older adults who are aging in place.</p><p><i>JAGS</i> has been at the forefront of rigorous examination of the community paramedicine model of care for older adults. As early as 1968, Mel Spear advocated for the concept of a physician-led, team-based, patient-centered approach to physical, emotional, and social well-being of older adults in “Paramedical Services for Older Adults.”<span><sup>6</sup></span> More recently, <i>JAGS</i> authors have described an array of community paramedicine programs tailored to the needs of older adults, including providing urgent, in-home, integrated evaluation and treatment to avoid unnecessary EMS transportation of medically complex older adults,<span><sup>7, 8</sup></span> facilitating the ED-to-home care transition,<span><sup>9</sup></span> using 9-1-1 calls as a sentinel event to prompt fall prevention intervention,<span><sup>10, 11</sup></span> and integrating community paramedics into home-based primary care practices to extend telehealth geriatrician reach and efficiency.<span><sup>12</sup></span> Additional program examples support the feasibility, effectiveness, and short-term health outcomes of community paramedicine for older adults.<span><sup>13-15</sup></span> However, limited data describe patient safety, process and health outcomes, and sustainable financial models for community paramedicine (Figure 1).</p><p>In this issue of <i>JAGS</i>, Parsons et al. examine a common clinical dilemma affecting the care of older adults: how does a clinician balance the need to evaluate a community-dwelling older adult with dementia and an unscheduled acute care need, with the risk of iatrogenic harm associated with exposure to and transitioning to-and-from an acute care facility for evaluation? The authors leveraged a community paramedicine service available to their home-based primary care teams to provide older adults the benefit of timely access to care without defaulting to the risks of the traditional unscheduled acute care paradigm. Beyond achieving their primary aim of demonstrating the safety of community paramedicine intervention for older adults with dementia, the authors noted three pertinent findings applicable to the broader field of geriatrics.</p><p>The authors noted increased economic and racial diversity among their community paramedicine program participants with dementia. This is infrequently reported on in the community paramedicine literature but sheds an important light on community paramedicine programs as a community health service capable of promoting health equity and trust.<span><sup>16</sup></span> Furthermore, among patients evaluated by the community paramedicine program, those with dementia were more likely to be referred to hospice. While not the primary outcome of this study, this finding highlights the potential of community paramedicine programs to alter clinical trajectories for patients who would historically end up in the revolving door of acute care use near the end of life. This unique finding adds to a growing literature base supporting the ability of community paramedicine programs to leverage an in-home acute care evaluation to prompt appropriate referrals and wrap-around services, as previously demonstrated for conditions such as falls and fragility fractures.<span><sup>10, 11</sup></span> Finally, this model of care leveraged multiple funding sources: value-based care as part of a health system accountable care organization, telemedicine visit reimbursement, and volume-based billing to build upon the predominantly single-source funding used in the other community paramedicine programs highlighted above. Though the study was limited in its use of a novel outcome (over vs under-transport) that will require additional validation and generalizability limited to home-based primary care practices, this study contributes to the growing literature base supporting community paramedicine for older adults.</p><p>With mounting evidence that integrated, in-home care for older adults through community paramedicine is safe, acceptable, and effective, what barriers limit expansion?</p><p>First, there remains a flashing lights and sirens conceptualization of EMS that emphasizes its traditional transportation role. While this is certainly a popular perception, it misses the fact that EMS clinicians are trained medical professionals embedded in communities across the nation with the ability to provide a wide spectrum of mobile and in-home care. Because of this, opportunities for collaboration between EMS agencies and nonemergency specialties often go unrecognized and underutilized in caring for older adults. In addition to limited awareness of community paramedicine partners, concerns regarding duplication of services also stifle growth. Early guidelines from the National Association of State EMS Officials recommend using a community health needs assessment to identify gaps in care that would best be addressed by community paramedics.<span><sup>17</sup></span></p><p>Second, EMS agencies are largely regulated at the local and state level. In some cases, flexible regulations promote locally tailored solutions that led to many of the innovative community paramedicine programs highlighted above. In other cases, rigid regulations may standardize the approach but reduce the ability to customize a program to adapt to community needs.<span><sup>18</sup></span> This variation in practice leads to challenges in both training and outcomes reporting. Heterogeneity in the services offered and variety of EMS clinicians performing these roles (e.g., emergency medical technician, advanced emergency medical technician, paramedic), the National EMS Advisory Council recommended ongoing consensus development regarding education requirements for an expanded role of EMS clinicians before establishing a national standard.<span><sup>19</sup></span> Similarly, variations in program design and outcomes reporting make it difficult to conduct the rigorous research necessary to inform policy development.</p><p>Third, collaboration between EMS agencies and nonemergency specialties requires the ability to see, share, and synchronize data. Many EMS agencies struggle to establish the complex, and often expensive, linkage and health records access from multiple sources. While some EMS agencies have circumvented the issue via health systems partnerships with accessible electronic health records, this barrier is notably high for smaller EMS agencies, clinician practices, and health systems alike.</p><p>Finally, payment for both community paramedicine programs and multidisciplinary care for older adults remains problematic. Despite promising international examples of cost reduction and improved health outcomes through community paramedicine, reimbursement for EMS-based services in the United States has largely depended upon transporting a patient rather than the value of the care provided and outcomes achieved.<span><sup>14, 20</sup></span> As such, many community paramedicine programs are grant-funded or subsidized by a health system, though more recent policies have explored fee-for-service and value-based payments. However, the lack of reimbursement for both the care provided and outcomes achieved remains threatening to the field as a whole.<span><sup>15</sup></span> We echo the sentiments of Colenda and Applegate and believe that their proposed solution of increasing investment in geriatric clinical service lines should include funding community paramedicine programs for older adults.<span><sup>2</sup></span></p><p>Leveraging integrated primary care and community paramedicine partnerships, as outlined in Parsons et al., demonstrates that team-based, mobile, patient-centered approaches can fill critical gaps in care, promote health equity, and alter the trajectory of older adults' care to promote aging in place. We encourage you to read Parsons et al.'s paper in this issue of <i>JAGS</i>, consider EMS agencies and clinicians beyond the lights and sirens, and re-envision EMS as a critical partner in transforming care delivery for older adults.</p><p><i>Concept, design, and writing</i>: Alexander J. Ulintz and Carmen E. Quatman.</p><p>The authors declare no conflicts of interest relevant to this study.</p><p>The sponsors had no role in any aspect of the research or preparation or approval of the manuscript.</p>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 9","pages":"2640-2643"},"PeriodicalIF":4.5000,"publicationDate":"2024-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19087","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19087","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Providing unscheduled, acute, and longitudinal care to older adults who are aging in place is a critical, yet largely unsolved, health system challenge. A large gap exists between the times and places where older adults need care and the resources available to address those needs.1 Despite efforts to increase older adults' access to in-home care through home-based primary care, telemedicine, and workforce development, persistent gaps prompted recent calls by the American Geriatrics Society and the American Association of Geriatric Psychiatry to expand the “team based geriatric physician and health professional workforce by nontraditional means.”2, 3 This creates an opportunity for innovative, multidisciplinary, patient-centered teams to bridge the gap.
Emergency medical services (EMS) agencies and clinicians are often called upon to fill this gap: they are accessible, mobile, and a trusted source of care in communities across the nation.4 Though originally designed for emergency treatment and transportation of the critically ill and injured, EMS clinicians are increasingly embracing roles that span community outreach, prevention, and chronic disease management in a model of care known as “community paramedicine.”5 Community paramedicine is designed to fill the space between fixed medical system resources and dynamic community needs by leveraging availability, accessibility, and versatile skills of EMS clinicians working as part of physician-led or multidisciplinary team. This model of care is of clear importance to older adults who are aging in place.
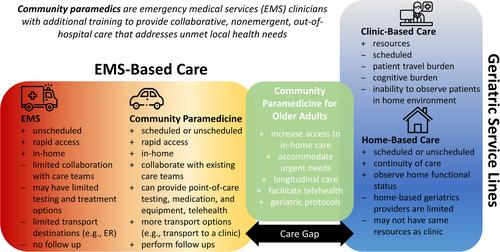
JAGS has been at the forefront of rigorous examination of the community paramedicine model of care for older adults. As early as 1968, Mel Spear advocated for the concept of a physician-led, team-based, patient-centered approach to physical, emotional, and social well-being of older adults in “Paramedical Services for Older Adults.”6 More recently, JAGS authors have described an array of community paramedicine programs tailored to the needs of older adults, including providing urgent, in-home, integrated evaluation and treatment to avoid unnecessary EMS transportation of medically complex older adults,7, 8 facilitating the ED-to-home care transition,9 using 9-1-1 calls as a sentinel event to prompt fall prevention intervention,10, 11 and integrating community paramedics into home-based primary care practices to extend telehealth geriatrician reach and efficiency.12 Additional program examples support the feasibility, effectiveness, and short-term health outcomes of community paramedicine for older adults.13-15 However, limited data describe patient safety, process and health outcomes, and sustainable financial models for community paramedicine (Figure 1).
In this issue of JAGS, Parsons et al. examine a common clinical dilemma affecting the care of older adults: how does a clinician balance the need to evaluate a community-dwelling older adult with dementia and an unscheduled acute care need, with the risk of iatrogenic harm associated with exposure to and transitioning to-and-from an acute care facility for evaluation? The authors leveraged a community paramedicine service available to their home-based primary care teams to provide older adults the benefit of timely access to care without defaulting to the risks of the traditional unscheduled acute care paradigm. Beyond achieving their primary aim of demonstrating the safety of community paramedicine intervention for older adults with dementia, the authors noted three pertinent findings applicable to the broader field of geriatrics.
The authors noted increased economic and racial diversity among their community paramedicine program participants with dementia. This is infrequently reported on in the community paramedicine literature but sheds an important light on community paramedicine programs as a community health service capable of promoting health equity and trust.16 Furthermore, among patients evaluated by the community paramedicine program, those with dementia were more likely to be referred to hospice. While not the primary outcome of this study, this finding highlights the potential of community paramedicine programs to alter clinical trajectories for patients who would historically end up in the revolving door of acute care use near the end of life. This unique finding adds to a growing literature base supporting the ability of community paramedicine programs to leverage an in-home acute care evaluation to prompt appropriate referrals and wrap-around services, as previously demonstrated for conditions such as falls and fragility fractures.10, 11 Finally, this model of care leveraged multiple funding sources: value-based care as part of a health system accountable care organization, telemedicine visit reimbursement, and volume-based billing to build upon the predominantly single-source funding used in the other community paramedicine programs highlighted above. Though the study was limited in its use of a novel outcome (over vs under-transport) that will require additional validation and generalizability limited to home-based primary care practices, this study contributes to the growing literature base supporting community paramedicine for older adults.
With mounting evidence that integrated, in-home care for older adults through community paramedicine is safe, acceptable, and effective, what barriers limit expansion?
First, there remains a flashing lights and sirens conceptualization of EMS that emphasizes its traditional transportation role. While this is certainly a popular perception, it misses the fact that EMS clinicians are trained medical professionals embedded in communities across the nation with the ability to provide a wide spectrum of mobile and in-home care. Because of this, opportunities for collaboration between EMS agencies and nonemergency specialties often go unrecognized and underutilized in caring for older adults. In addition to limited awareness of community paramedicine partners, concerns regarding duplication of services also stifle growth. Early guidelines from the National Association of State EMS Officials recommend using a community health needs assessment to identify gaps in care that would best be addressed by community paramedics.17
Second, EMS agencies are largely regulated at the local and state level. In some cases, flexible regulations promote locally tailored solutions that led to many of the innovative community paramedicine programs highlighted above. In other cases, rigid regulations may standardize the approach but reduce the ability to customize a program to adapt to community needs.18 This variation in practice leads to challenges in both training and outcomes reporting. Heterogeneity in the services offered and variety of EMS clinicians performing these roles (e.g., emergency medical technician, advanced emergency medical technician, paramedic), the National EMS Advisory Council recommended ongoing consensus development regarding education requirements for an expanded role of EMS clinicians before establishing a national standard.19 Similarly, variations in program design and outcomes reporting make it difficult to conduct the rigorous research necessary to inform policy development.
Third, collaboration between EMS agencies and nonemergency specialties requires the ability to see, share, and synchronize data. Many EMS agencies struggle to establish the complex, and often expensive, linkage and health records access from multiple sources. While some EMS agencies have circumvented the issue via health systems partnerships with accessible electronic health records, this barrier is notably high for smaller EMS agencies, clinician practices, and health systems alike.
Finally, payment for both community paramedicine programs and multidisciplinary care for older adults remains problematic. Despite promising international examples of cost reduction and improved health outcomes through community paramedicine, reimbursement for EMS-based services in the United States has largely depended upon transporting a patient rather than the value of the care provided and outcomes achieved.14, 20 As such, many community paramedicine programs are grant-funded or subsidized by a health system, though more recent policies have explored fee-for-service and value-based payments. However, the lack of reimbursement for both the care provided and outcomes achieved remains threatening to the field as a whole.15 We echo the sentiments of Colenda and Applegate and believe that their proposed solution of increasing investment in geriatric clinical service lines should include funding community paramedicine programs for older adults.2
Leveraging integrated primary care and community paramedicine partnerships, as outlined in Parsons et al., demonstrates that team-based, mobile, patient-centered approaches can fill critical gaps in care, promote health equity, and alter the trajectory of older adults' care to promote aging in place. We encourage you to read Parsons et al.'s paper in this issue of JAGS, consider EMS agencies and clinicians beyond the lights and sirens, and re-envision EMS as a critical partner in transforming care delivery for older adults.
Concept, design, and writing: Alexander J. Ulintz and Carmen E. Quatman.
The authors declare no conflicts of interest relevant to this study.
The sponsors had no role in any aspect of the research or preparation or approval of the manuscript.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
