{"title":"Commentary on: Cost-effectiveness of pneumococcal vaccination and of programs to increase its uptake in U.S. older adults","authors":"Melissa K. Andrew MD, PhD","doi":"10.1111/jgs.19079","DOIUrl":null,"url":null,"abstract":"<p>Pneumococcal illness, including both invasive disease and pneumonia, is especially relevant for older adults. Notably, the burden of disease increases with age, as does the risk of adverse outcomes which include both short- and long-term sequalae.<span><sup>1-8</sup></span> Several pneumococcal vaccines are currently available, including conjugate (PCV) and polysaccharide (PPV) vaccines covering different numbers of pneumococcal serotypes chosen to represent those causing the greatest burden of severe illness. Current both ACIP (the US Advisory Committee on Immunization Practices) and NACI (Canada's National Advisory Committee on Immunization) recommend PCV20 (or PCV15 + PPV23) for adults aged 65+ or with certain high-risk conditions.<span><sup>9, 10</sup></span></p><p>Despite older adults being among the groups most in need of protection, the benefit they derive from vaccines to date has been suboptimal, because of two issues: (1) suboptimal vaccine effectiveness (VE) in older adults due to immune dysregulation (in which efforts to tailor vaccine product composition, e.g. dose and adjuvants, and their delivery, e.g. dosing intervals, and number of doses, may be helpful) and (2) suboptimal uptake of vaccines that are recommended and available.<span><sup>11</sup></span> Targets for vaccine coverage in adults vary by jurisdiction, but a target of 80% is often put forth for pneumococcal vaccine coverage in older adults and adults with high-risk conditions.</p><p>When we further explore the suboptimal immunization coverage seen for all older adults, people in population groups facing historical and present social and structural disadvantage, and those in racialized groups, tend to experience compounded barriers in access and uptake to preventative interventions including vaccination.<span><sup>12-14</sup></span> It is therefore important to consider whether programs developed with and for these communities will be beneficial in achieving better vaccination uptake.</p><p>In the current issue, Wateska et al. present a study examining cost-effectiveness of pneumococcal vaccination for older adults and targeted programs to increase its uptake.<span><sup>15</sup></span> They used Markov decision analysis models comparing hypothetical one-year age band cohorts of Black and non-Black US adults aged 65 years and compared strategies of no vaccination, vaccination per current ACIP/CDC guidelines, and vaccination plus implementation of a program aiming to increase vaccine uptake.</p><p>They found that adult pneumococcal programs using PCV20 or PCV15 + PPV23 targeting a cross-sectional single year cohort of older adults 65 years of age are unlikely to be cost-effective, with all options having Incremental Cost-Effectiveness Ratios (ICERs) of more than $200,000 per Quality Adjusted Life Year (QALY). The authors conducted probabilistic sensitivity analyses varying many of the model assumptions and still found that these were unlikely to be cost-effective at thresholds of $200,000/QALY in those aged 65.</p><p>The authors point out that the successful protection from vaccines is highly dependent on vaccine confidence and uptake, and so the present analysis included consideration of the impact of two versions of programs to enhance uptake—one modeling a program targeted to Black older adults, and one that would target non-Black older adults, aiming to address racial differences in disease risk and vaccine confidence/uptake. Programs costing $2.19 per vaccine-eligible person were assumed to increase uptake by 7.5% (which was varied from 0 to 20% in sensitivity analyses). They found that economic models including these programs still showed unfavorable cost-effectiveness.</p><p>Wateska et al. argue that accounting for (likely) enhanced herd immunity relating to use of these newer pneumococcal vaccines (PCV20 and PCV15) in children would tend to make the cost-effectiveness of their use in older adults even more unfavorable. While emphasizing the importance of continued childhood vaccination for indirect benefit in older adults, they suggest that a vaccine strategy that targets serotypes that are not contained in the childhood vaccines but that are more burdensome to older adults could be clinically and economically favorable. They point out that such vaccines are currently being investigated, which raises the interesting question of whether a vaccine specifically targeted to the unique pneumococcal serotypes that cause more disease in adults could be a more cost-effective strategy.</p><p>This analysis is helpful in providing some context for decision-making around potential introduction or expansion of adult pneumococcal vaccination programs and targeted efforts to increase vaccine uptake. At first glance, it is sobering to see that the programs studied in the base case do not appear to be cost-effective, with ICER >$200,000 USD per QALY. Even so, from a policy and programmatic standpoint, it would be unlikely to see a vaccine recommendation for use of PCV vaccines in a single year age band (age 65) of older adults, which is the base case presented by Wateska et al. and the subject of nearly all of the article's analyses.</p><p>Recognizing that pneumococcal disease risk increases with increasing age, they conducted a subset of additional analyses aiming to address the question of whether and how vaccination programs including adults older than 65, or using and older age cutoff, would impact cost-effectiveness. In these analyses they also account for expected lower vaccine effectiveness with increasing age. Simultaneously varying pneumococcal disease risk and VE, they found that a PCV20 program could be considered cost-effective at a threshold of $200,000/QALY if the disease risk was 40%–60% greater than that experienced by the 65–79 year olds. This analysis, presented in Supplemental Figure S4, is critically important in informing a nuanced interpretation of this question, because vaccine programs are unlikely to target a single year age band, particularly the one at lowest risk of the illness in the age group for whom vaccination is recommended where cost-effectiveness is thus likely to be least favorable. Given that risk increases continuously but nonlinearly with increasing age, even within the 65–79 year age group, it is important to consider whether vaccination programs utilizing a higher age cutoff could be more cost-effective. (Figure 1) Additionally, given that risk among older adults derives not only from chronological age, but also from health conditions and frailty that are heterogeneously experienced, tailoring vaccination strategies for populations with highest risk within the older adult age groups remains another important option for further study.</p><p>Even though age and frailty are increasingly understood to be relevant for respiratory infection burden of illness and vaccine effectiveness, many knowledge gaps remain.<span><sup>16-18</sup></span> There may also be sex differences in aging immune responses.<span><sup>19</sup></span> Overall, more work is required on immunogenicity and vaccine effectiveness in relation to age and frailty and on duration of protection of these vaccines in older adults and those living with high-risk conditions or frailty. As a practical example, if people with high-risk conditions receive a vaccine at a younger age, how long does this protection last?</p><p>Wateska et al.'s article is topically relevant given recent updated recommendations on use of Pneumococcal vaccination in older adults by ACIP and other international immunization technical advisory groups. Although the base case models of implementing pneumococcal vaccination in 65 year olds, with or without programs to enhance uptake, do not appear to be cost-effective, their additional analyses suggest two potential approaches that would benefit from further consideration: (1) implementation in older age groups or higher risk populations, and/or (2) vaccines tailored to include the unique pneumococcal serotypes that are most burdensome for older adults in the presence of indirect benefit from childhood programs.</p><p>Such efforts will be important so that immunization advisory groups and policy-makers are able to have the strongest evidence base from which to consider the potential benefits and cost-effectiveness of different age-based recommendations or tailored programs to increase uptake and enhance protection of the most vulnerable populations.</p><p>MKA is the sole contributor.</p><p>MKA reports grants from Sanofi, GSK, Merck, and Pfizer for research studies relating to vaccine preventable illnesses in older adults and is a member of Canada's National Advisory Committee on Immunization.</p><p>The present article is unfunded.</p>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 8","pages":"2299-2302"},"PeriodicalIF":4.5000,"publicationDate":"2024-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19079","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19079","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Pneumococcal illness, including both invasive disease and pneumonia, is especially relevant for older adults. Notably, the burden of disease increases with age, as does the risk of adverse outcomes which include both short- and long-term sequalae.1-8 Several pneumococcal vaccines are currently available, including conjugate (PCV) and polysaccharide (PPV) vaccines covering different numbers of pneumococcal serotypes chosen to represent those causing the greatest burden of severe illness. Current both ACIP (the US Advisory Committee on Immunization Practices) and NACI (Canada's National Advisory Committee on Immunization) recommend PCV20 (or PCV15 + PPV23) for adults aged 65+ or with certain high-risk conditions.9, 10
Despite older adults being among the groups most in need of protection, the benefit they derive from vaccines to date has been suboptimal, because of two issues: (1) suboptimal vaccine effectiveness (VE) in older adults due to immune dysregulation (in which efforts to tailor vaccine product composition, e.g. dose and adjuvants, and their delivery, e.g. dosing intervals, and number of doses, may be helpful) and (2) suboptimal uptake of vaccines that are recommended and available.11 Targets for vaccine coverage in adults vary by jurisdiction, but a target of 80% is often put forth for pneumococcal vaccine coverage in older adults and adults with high-risk conditions.
When we further explore the suboptimal immunization coverage seen for all older adults, people in population groups facing historical and present social and structural disadvantage, and those in racialized groups, tend to experience compounded barriers in access and uptake to preventative interventions including vaccination.12-14 It is therefore important to consider whether programs developed with and for these communities will be beneficial in achieving better vaccination uptake.
In the current issue, Wateska et al. present a study examining cost-effectiveness of pneumococcal vaccination for older adults and targeted programs to increase its uptake.15 They used Markov decision analysis models comparing hypothetical one-year age band cohorts of Black and non-Black US adults aged 65 years and compared strategies of no vaccination, vaccination per current ACIP/CDC guidelines, and vaccination plus implementation of a program aiming to increase vaccine uptake.
They found that adult pneumococcal programs using PCV20 or PCV15 + PPV23 targeting a cross-sectional single year cohort of older adults 65 years of age are unlikely to be cost-effective, with all options having Incremental Cost-Effectiveness Ratios (ICERs) of more than $200,000 per Quality Adjusted Life Year (QALY). The authors conducted probabilistic sensitivity analyses varying many of the model assumptions and still found that these were unlikely to be cost-effective at thresholds of $200,000/QALY in those aged 65.
The authors point out that the successful protection from vaccines is highly dependent on vaccine confidence and uptake, and so the present analysis included consideration of the impact of two versions of programs to enhance uptake—one modeling a program targeted to Black older adults, and one that would target non-Black older adults, aiming to address racial differences in disease risk and vaccine confidence/uptake. Programs costing $2.19 per vaccine-eligible person were assumed to increase uptake by 7.5% (which was varied from 0 to 20% in sensitivity analyses). They found that economic models including these programs still showed unfavorable cost-effectiveness.
Wateska et al. argue that accounting for (likely) enhanced herd immunity relating to use of these newer pneumococcal vaccines (PCV20 and PCV15) in children would tend to make the cost-effectiveness of their use in older adults even more unfavorable. While emphasizing the importance of continued childhood vaccination for indirect benefit in older adults, they suggest that a vaccine strategy that targets serotypes that are not contained in the childhood vaccines but that are more burdensome to older adults could be clinically and economically favorable. They point out that such vaccines are currently being investigated, which raises the interesting question of whether a vaccine specifically targeted to the unique pneumococcal serotypes that cause more disease in adults could be a more cost-effective strategy.
This analysis is helpful in providing some context for decision-making around potential introduction or expansion of adult pneumococcal vaccination programs and targeted efforts to increase vaccine uptake. At first glance, it is sobering to see that the programs studied in the base case do not appear to be cost-effective, with ICER >$200,000 USD per QALY. Even so, from a policy and programmatic standpoint, it would be unlikely to see a vaccine recommendation for use of PCV vaccines in a single year age band (age 65) of older adults, which is the base case presented by Wateska et al. and the subject of nearly all of the article's analyses.
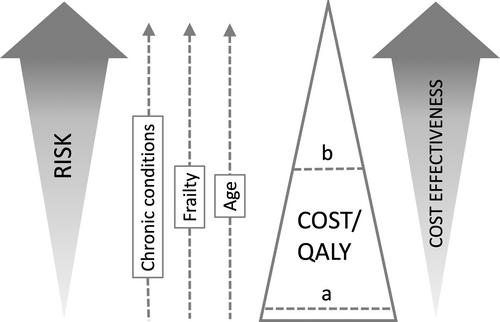
Recognizing that pneumococcal disease risk increases with increasing age, they conducted a subset of additional analyses aiming to address the question of whether and how vaccination programs including adults older than 65, or using and older age cutoff, would impact cost-effectiveness. In these analyses they also account for expected lower vaccine effectiveness with increasing age. Simultaneously varying pneumococcal disease risk and VE, they found that a PCV20 program could be considered cost-effective at a threshold of $200,000/QALY if the disease risk was 40%–60% greater than that experienced by the 65–79 year olds. This analysis, presented in Supplemental Figure S4, is critically important in informing a nuanced interpretation of this question, because vaccine programs are unlikely to target a single year age band, particularly the one at lowest risk of the illness in the age group for whom vaccination is recommended where cost-effectiveness is thus likely to be least favorable. Given that risk increases continuously but nonlinearly with increasing age, even within the 65–79 year age group, it is important to consider whether vaccination programs utilizing a higher age cutoff could be more cost-effective. (Figure 1) Additionally, given that risk among older adults derives not only from chronological age, but also from health conditions and frailty that are heterogeneously experienced, tailoring vaccination strategies for populations with highest risk within the older adult age groups remains another important option for further study.
Even though age and frailty are increasingly understood to be relevant for respiratory infection burden of illness and vaccine effectiveness, many knowledge gaps remain.16-18 There may also be sex differences in aging immune responses.19 Overall, more work is required on immunogenicity and vaccine effectiveness in relation to age and frailty and on duration of protection of these vaccines in older adults and those living with high-risk conditions or frailty. As a practical example, if people with high-risk conditions receive a vaccine at a younger age, how long does this protection last?
Wateska et al.'s article is topically relevant given recent updated recommendations on use of Pneumococcal vaccination in older adults by ACIP and other international immunization technical advisory groups. Although the base case models of implementing pneumococcal vaccination in 65 year olds, with or without programs to enhance uptake, do not appear to be cost-effective, their additional analyses suggest two potential approaches that would benefit from further consideration: (1) implementation in older age groups or higher risk populations, and/or (2) vaccines tailored to include the unique pneumococcal serotypes that are most burdensome for older adults in the presence of indirect benefit from childhood programs.
Such efforts will be important so that immunization advisory groups and policy-makers are able to have the strongest evidence base from which to consider the potential benefits and cost-effectiveness of different age-based recommendations or tailored programs to increase uptake and enhance protection of the most vulnerable populations.
MKA is the sole contributor.
MKA reports grants from Sanofi, GSK, Merck, and Pfizer for research studies relating to vaccine preventable illnesses in older adults and is a member of Canada's National Advisory Committee on Immunization.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
