Thomas Akel Oberpaur, Tania M. Capusan, Ana R. Gamero Rodríguez, Iván Rodrigo Díaz, Javier Alcántara González, Marta Ruano Del Salado, Cristian Perna, Carla Rodríguez Naranjo, María Elena Sánchez-Largo Uceda
{"title":"Itchy vesicles on black skin","authors":"Thomas Akel Oberpaur, Tania M. Capusan, Ana R. Gamero Rodríguez, Iván Rodrigo Díaz, Javier Alcántara González, Marta Ruano Del Salado, Cristian Perna, Carla Rodríguez Naranjo, María Elena Sánchez-Largo Uceda","doi":"10.1002/jvc2.485","DOIUrl":null,"url":null,"abstract":"<p>A 60-year-old black woman from Ghana, who had been residing in Spain for over 20 years, was referred to our clinic after presenting progressively itchy lesions following a unilateral knee replacement surgery 4 months ago. Her medical background was notable for obesity, osteoarthritis, hypertension and hypothyroidism. The patient noted the onset of her symptoms once the postoperative pain had subsided. At first, pruritus and dark macules around the scars were believed to be normal but then continued to develop scaly, and itchy plaques predominantly on the extensor surfaces of both her lower limbs. These plaques gradually progressed to cover her back and trunk, sparing the face and mucous membranes. Her condition had not improved with empiric topical corticosteroids before our evaluation.</p><p>Upon dermatological examination, she exhibited multiple clear vesicles on erosive, pruritic, lichenified and hyperpigmented plaques (Figure 1). These vesicles were noteworthy for not being fragile or entirely flaccid. Certain blood tests were ordered and an intact vesicle and surrounding skin were excised for microscopic investigation (Figure 2).</p><p>PF is a rare subtype of pemphigus, much less frequently encountered than pemphigus vulgaris (PV). It is uncommon globally, with a higher prevalence in endemic areas like Brazil and Africa, more related to geographic and socioeconomic factors rather than ethnicity, age or gender.<span><sup>1</sup></span> The literature on PF cases in individuals from Africa is limited, though there is a noted higher incidence in South Africa<span><sup>2</sup></span> and endemic occurrences in the northern African countries and the Kilimanjaro region<span><sup>3</sup></span> (namely Kenya and Tanzania). Our case exemplifies a sporadic (nonendemic) occurrence of PF, with no related geographical, travel or medication history. Even though triggers are not usually identified, this case seems to have been triggered by the surgery, which has been reported in some other publications.</p><p>PF's typical presentation involves painful scaly, erythematous erosions in seborrheic areas, with intact vesicles being a rare find.<span><sup>4, 5</sup></span> Our case diverges from the norm, as the patient has never noted pain regarding this condition, seborrheic areas are spared at every flare-up and vesicles remain intact for several days. The presence of circulating antibodies targeting Dsg-1, a necessary adhesion molecule in the outer layers of cutaneos epidermis but not indispensable in mucosas, along with preservation of Dsg-3, reflect the physiopathology of this disease and the differences with PV.<span><sup>5</sup></span> Although we cannot establish why the distribution or the symptoms in our case differs from the classic presentation, we can at least hypothesize that the vesicles are less fragile owing to the more compact corneal layer found in black skin.<span><sup>6</sup></span> Interestingly, the notorious postinflammatory hyperpigmentation and lack of erythema in the dark-skinned individuals can sometimes mislead the clinician if the vesicles are not detected, which has to be taken into account when examining different skin tones.</p><p>Treatments for PF are the same as those known for PV. Our patient responded well to systemic corticosteroids but has been unable to discontinue them even after the introduction of azathioprine. She is contemplating the possibility of receiving rituximab, an excellent option and considered a first-line treatment as per the evidence in recent years.</p><p>This case adds to a growing pool of clinical aspects of skin diseases in individuals with black skin, a demographic often underrepresented in dermatology. Training our diagnostic accuracy in different skin phenotypes is a must.</p><p><i>Conception of manuscript and main caregivers</i>: Thomas Akel-Oberpaur and Tania M. Capusan. <i>Histology</i>: Cristian Perna and Carla Rodríguez Naranjo. <i>Substantial contributions to design, acquisition of data and critically revising intellectual content</i>: Ana R. Gamero Rodríguez, Javier Alcántara González, Marta Ruano Del Salado and Iván Rodrigo Díaz. <i>Final approval of the version to be published</i>: Thomas Akel-Oberpaur and María Elena Sánchez-Largo Uceda.</p><p>The authors declare no conflict of interest.</p><p>The patient in this manuscript has given written informed consent for participation in the study and the use of their de-identified, anonymized, aggregated data and their case details (including photographs) for publication. Ethical Approval: not applicable.</p>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 3","pages":"934-937"},"PeriodicalIF":0.5000,"publicationDate":"2024-07-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.485","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.485","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
A 60-year-old black woman from Ghana, who had been residing in Spain for over 20 years, was referred to our clinic after presenting progressively itchy lesions following a unilateral knee replacement surgery 4 months ago. Her medical background was notable for obesity, osteoarthritis, hypertension and hypothyroidism. The patient noted the onset of her symptoms once the postoperative pain had subsided. At first, pruritus and dark macules around the scars were believed to be normal but then continued to develop scaly, and itchy plaques predominantly on the extensor surfaces of both her lower limbs. These plaques gradually progressed to cover her back and trunk, sparing the face and mucous membranes. Her condition had not improved with empiric topical corticosteroids before our evaluation.
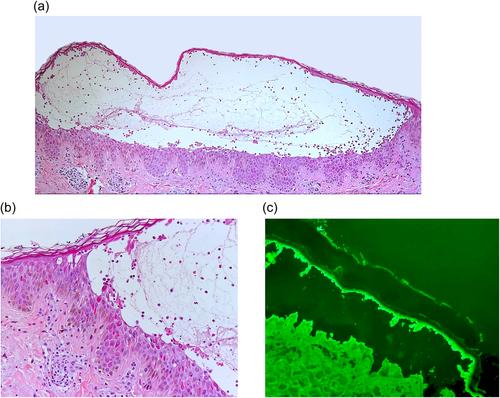
Upon dermatological examination, she exhibited multiple clear vesicles on erosive, pruritic, lichenified and hyperpigmented plaques (Figure 1). These vesicles were noteworthy for not being fragile or entirely flaccid. Certain blood tests were ordered and an intact vesicle and surrounding skin were excised for microscopic investigation (Figure 2).
PF is a rare subtype of pemphigus, much less frequently encountered than pemphigus vulgaris (PV). It is uncommon globally, with a higher prevalence in endemic areas like Brazil and Africa, more related to geographic and socioeconomic factors rather than ethnicity, age or gender.1 The literature on PF cases in individuals from Africa is limited, though there is a noted higher incidence in South Africa2 and endemic occurrences in the northern African countries and the Kilimanjaro region3 (namely Kenya and Tanzania). Our case exemplifies a sporadic (nonendemic) occurrence of PF, with no related geographical, travel or medication history. Even though triggers are not usually identified, this case seems to have been triggered by the surgery, which has been reported in some other publications.
PF's typical presentation involves painful scaly, erythematous erosions in seborrheic areas, with intact vesicles being a rare find.4, 5 Our case diverges from the norm, as the patient has never noted pain regarding this condition, seborrheic areas are spared at every flare-up and vesicles remain intact for several days. The presence of circulating antibodies targeting Dsg-1, a necessary adhesion molecule in the outer layers of cutaneos epidermis but not indispensable in mucosas, along with preservation of Dsg-3, reflect the physiopathology of this disease and the differences with PV.5 Although we cannot establish why the distribution or the symptoms in our case differs from the classic presentation, we can at least hypothesize that the vesicles are less fragile owing to the more compact corneal layer found in black skin.6 Interestingly, the notorious postinflammatory hyperpigmentation and lack of erythema in the dark-skinned individuals can sometimes mislead the clinician if the vesicles are not detected, which has to be taken into account when examining different skin tones.
Treatments for PF are the same as those known for PV. Our patient responded well to systemic corticosteroids but has been unable to discontinue them even after the introduction of azathioprine. She is contemplating the possibility of receiving rituximab, an excellent option and considered a first-line treatment as per the evidence in recent years.
This case adds to a growing pool of clinical aspects of skin diseases in individuals with black skin, a demographic often underrepresented in dermatology. Training our diagnostic accuracy in different skin phenotypes is a must.
Conception of manuscript and main caregivers: Thomas Akel-Oberpaur and Tania M. Capusan. Histology: Cristian Perna and Carla Rodríguez Naranjo. Substantial contributions to design, acquisition of data and critically revising intellectual content: Ana R. Gamero Rodríguez, Javier Alcántara González, Marta Ruano Del Salado and Iván Rodrigo Díaz. Final approval of the version to be published: Thomas Akel-Oberpaur and María Elena Sánchez-Largo Uceda.
The authors declare no conflict of interest.
The patient in this manuscript has given written informed consent for participation in the study and the use of their de-identified, anonymized, aggregated data and their case details (including photographs) for publication. Ethical Approval: not applicable.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
