Optimizing electrical efficacy of leadless cardiac resynchronization therapy and leadless left ventricular septal pacing: Insights on left and right ventricular activation from electrocardiographic imaging
Nadeev Wijesuriya MBBS , Marina Strocchi PhD , Mark Elliott MBBS, PhD , Vishal Mehta MBBS , Felicity De Vere MBBS , Sandra Howell MBBS , Nilanka Mannakkara MBBS , Baldeep S. Sidhu MBBS, PhD , Jane Kwan MSc , Paolo Bosco MBBS , Steven A. Niederer DPhil , Christopher A. Rinaldi MBBS, MD, FHRS
{"title":"Optimizing electrical efficacy of leadless cardiac resynchronization therapy and leadless left ventricular septal pacing: Insights on left and right ventricular activation from electrocardiographic imaging","authors":"Nadeev Wijesuriya MBBS , Marina Strocchi PhD , Mark Elliott MBBS, PhD , Vishal Mehta MBBS , Felicity De Vere MBBS , Sandra Howell MBBS , Nilanka Mannakkara MBBS , Baldeep S. Sidhu MBBS, PhD , Jane Kwan MSc , Paolo Bosco MBBS , Steven A. Niederer DPhil , Christopher A. Rinaldi MBBS, MD, FHRS","doi":"10.1016/j.hroo.2024.07.004","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Leadless cardiac resynchronization therapy (CRT) is an emerging heart failure treatment. An implanted electrode delivers lateral or septal endocardial left ventricular (LV) pacing (LVP) upon detection of a right ventricular (RV) pacing stimulus from a coimplanted device, thus generating biventricular pacing (BiVP). Electrical efficacy data regarding this therapy, particularly leadless LV septal pacing (LVSP) for potential conduction system capture, are limited.</p></div><div><h3>Objectives</h3><p>The purpose of this study was to evaluate the acute performance of leadless CRT using electrocardiographic imaging (ECGi) and assess the optimal pacing modality (OPM) of LVSP on the basis of RV and LV activation.</p></div><div><h3>Methods</h3><p>Ten WiSE-CRT recipients underwent an ECGi study testing: RV pacing, BiVP, LVP only, and LVP with an optimized atrioventricular delay (LV-OPT). BiV, LV, and RV activation times (shortest time taken to activate 90% of the ventricles [BIVAT-90], shortest time taken to activate 95% of the LV, and shortest time taken to activate 90% of the RV) plus LV and BiV dyssynchrony index (standard deviation of LV activation times and standard deviation of all activation times) were calculated from reconstructed epicardial electrograms. The individual OPM yielding the greatest improvement from baseline was determined.</p></div><div><h3>Results</h3><p>BiVP generated a 23.7% improvement in BiVAT-90 (<em>P</em> = .002). An improvement of 43.3% was observed at the OPM (<em>P</em> = .0001), primarily through reductions in shortest time taken to activate 90% of the RV. At the OPM, BiVAT-90 improved in patients with lateral (43.3%; <em>P</em> = .0001; n = 5) and septal (42.4%; <em>P</em> = .009; n = 5) LV implants. The OPM varied by individual. LVP and LV-OPT were mostly superior in patients with LVSP, and in those with sinus rhythm and left bundle branch block (n = 4).</p></div><div><h3>Conclusion</h3><p>Leadless CRT significantly improves acute ECGi-derived activation and dyssynchrony metrics. Using an individualized OPM improves efficacy in selected patients. Effective LVSP is feasible, with fusion pacing at LV-OPT mitigating the potential deleterious effects on RV activation.</p></div>","PeriodicalId":29772,"journal":{"name":"Heart Rhythm O2","volume":"5 8","pages":"Pages 551-560"},"PeriodicalIF":2.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2666501824002216/pdfft?md5=24bfc7b836daa1bb78f9e661a1efc301&pid=1-s2.0-S2666501824002216-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart Rhythm O2","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666501824002216","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/5 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Leadless cardiac resynchronization therapy (CRT) is an emerging heart failure treatment. An implanted electrode delivers lateral or septal endocardial left ventricular (LV) pacing (LVP) upon detection of a right ventricular (RV) pacing stimulus from a coimplanted device, thus generating biventricular pacing (BiVP). Electrical efficacy data regarding this therapy, particularly leadless LV septal pacing (LVSP) for potential conduction system capture, are limited.
Objectives
The purpose of this study was to evaluate the acute performance of leadless CRT using electrocardiographic imaging (ECGi) and assess the optimal pacing modality (OPM) of LVSP on the basis of RV and LV activation.
Methods
Ten WiSE-CRT recipients underwent an ECGi study testing: RV pacing, BiVP, LVP only, and LVP with an optimized atrioventricular delay (LV-OPT). BiV, LV, and RV activation times (shortest time taken to activate 90% of the ventricles [BIVAT-90], shortest time taken to activate 95% of the LV, and shortest time taken to activate 90% of the RV) plus LV and BiV dyssynchrony index (standard deviation of LV activation times and standard deviation of all activation times) were calculated from reconstructed epicardial electrograms. The individual OPM yielding the greatest improvement from baseline was determined.
Results
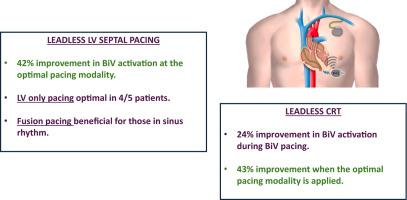
BiVP generated a 23.7% improvement in BiVAT-90 (P = .002). An improvement of 43.3% was observed at the OPM (P = .0001), primarily through reductions in shortest time taken to activate 90% of the RV. At the OPM, BiVAT-90 improved in patients with lateral (43.3%; P = .0001; n = 5) and septal (42.4%; P = .009; n = 5) LV implants. The OPM varied by individual. LVP and LV-OPT were mostly superior in patients with LVSP, and in those with sinus rhythm and left bundle branch block (n = 4).
Conclusion
Leadless CRT significantly improves acute ECGi-derived activation and dyssynchrony metrics. Using an individualized OPM improves efficacy in selected patients. Effective LVSP is feasible, with fusion pacing at LV-OPT mitigating the potential deleterious effects on RV activation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
