Renske Eveline Henriëtte Maria Bijl, Domenique Wilhelmina Antonia Maria Zaunbrecher, Petra Mathilda de Muynck, Ryanne Eggink, Ronique Timmer, Evian Willems, Sam Koning, Marieke Saskia Sanders, Kim Ellis Jie
{"title":"A multicenter retrospective cohort study on incidence and diagnostics in emergency department patients with acute vestibular syndrome.","authors":"Renske Eveline Henriëtte Maria Bijl, Domenique Wilhelmina Antonia Maria Zaunbrecher, Petra Mathilda de Muynck, Ryanne Eggink, Ronique Timmer, Evian Willems, Sam Koning, Marieke Saskia Sanders, Kim Ellis Jie","doi":"10.15441/ceem.24.225","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Acute vestibular syndrome (AVS) is a common symptom experienced by emergency department (ED) patients. Differentiating a peripheral from central etiology poses a challenge, and clinical practice lacks a uniform diagnostic approach. This study aims to provide insight on incidence and diagnostics in ED patients presenting with AVS in the Netherlands.</p><p><strong>Methods: </strong>This was a multicenter retrospective cohort study of ED patients presenting with AVS in one of two hospitals during a 3-year period. The primary endpoints were incidence, diagnostics, and diagnosis at ED presentation versus follow-up. The secondary endpoint was type of therapy.</p><p><strong>Results: </strong>Among the 500 AVS cases included, the annual incidence was 0.1%. Eighty-five ED patients (17.0%) were diagnosed with stroke, 285 (57.0%) did not experience stroke, and 130 (26.0%) exhibited an unsure etiology. At follow-up, diagnosis was revised in 145 patients (29.0%), with stroke missed in 29 (5.8%). A triad of clinical tests (head impulse test, observation of nystagmus, test of skew; HINTS) was completed for 106 patients (21.2%), computed tomography (CT) scans were collected in 342 patients (68.4%), and magnetic resonance imaging scans were collected for 153 patients (30.6%). Antiplatelet therapy was prescribed in 135 cases. In 69% of these, the initial diagnosis was revised to no stroke. Among eight patients who received thrombolysis, the initial diagnosis was revised for three. Of those patients in whom stroke was initially not identified, 23 (79%) received suboptimal treatment in lieu of antiplatelet therapy.</p><p><strong>Conclusion: </strong>The annual incidence of AVS in this Dutch ED cohort is 0.1%. ED diagnosis is often uncertain, with one-third of diagnoses later revised. This study substantiates that clinical practice lacks a uniform diagnostic pathway, with an overuse of CT imaging and underuse of HINTS. Further research on an optimal diagnostic approach is warranted to improve treatment of AVS.</p>","PeriodicalId":10325,"journal":{"name":"Clinical and Experimental Emergency Medicine","volume":" ","pages":"148-155"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12245650/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15441/ceem.24.225","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Acute vestibular syndrome (AVS) is a common symptom experienced by emergency department (ED) patients. Differentiating a peripheral from central etiology poses a challenge, and clinical practice lacks a uniform diagnostic approach. This study aims to provide insight on incidence and diagnostics in ED patients presenting with AVS in the Netherlands.
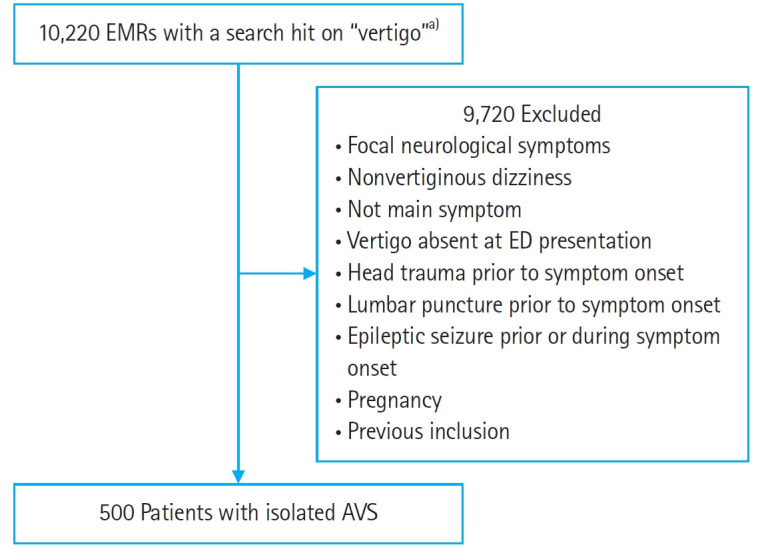
Methods: This was a multicenter retrospective cohort study of ED patients presenting with AVS in one of two hospitals during a 3-year period. The primary endpoints were incidence, diagnostics, and diagnosis at ED presentation versus follow-up. The secondary endpoint was type of therapy.
Results: Among the 500 AVS cases included, the annual incidence was 0.1%. Eighty-five ED patients (17.0%) were diagnosed with stroke, 285 (57.0%) did not experience stroke, and 130 (26.0%) exhibited an unsure etiology. At follow-up, diagnosis was revised in 145 patients (29.0%), with stroke missed in 29 (5.8%). A triad of clinical tests (head impulse test, observation of nystagmus, test of skew; HINTS) was completed for 106 patients (21.2%), computed tomography (CT) scans were collected in 342 patients (68.4%), and magnetic resonance imaging scans were collected for 153 patients (30.6%). Antiplatelet therapy was prescribed in 135 cases. In 69% of these, the initial diagnosis was revised to no stroke. Among eight patients who received thrombolysis, the initial diagnosis was revised for three. Of those patients in whom stroke was initially not identified, 23 (79%) received suboptimal treatment in lieu of antiplatelet therapy.
Conclusion: The annual incidence of AVS in this Dutch ED cohort is 0.1%. ED diagnosis is often uncertain, with one-third of diagnoses later revised. This study substantiates that clinical practice lacks a uniform diagnostic pathway, with an overuse of CT imaging and underuse of HINTS. Further research on an optimal diagnostic approach is warranted to improve treatment of AVS.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
