Ariana Barkley, Laura Lander, Brian Dilcher, Meghan Tuscano
{"title":"Initiation of Buprenorphine in the Emergency Department: A Survey of Emergency Clinicians.","authors":"Ariana Barkley, Laura Lander, Brian Dilcher, Meghan Tuscano","doi":"10.5811/westjem.18029","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Initiation of buprenorphine for opioid use disorder (OUD) in the emergency department (ED) is supported by the American College of Emergency Physicians and is shown to be beneficial. This practice, however, is largely underutilized.</p><p><strong>Methods: </strong>To assess emergency clinicians' attitudes and readiness to initiate buprenorphine in the ED we conducted a cross-sectional, electronic survey of clinicians (attendings, residents, and non-physician clinicians) in a single, academic ED of a tertiary-care hospital, which serves a rural population. Our survey aimed to assess emergency clinicians' attitudes toward and readiness to initiate buprenorphine in the ED and identify clinician-perceived facilitators and barriers. Our survey took place after the initiation of the IMPACT (Initiation of Medication, Peer Access, and Connection to Treatment) project.</p><p><strong>Results: </strong>Our results demonstrated the level of agreement that buprenorphine prescribing is within the emergency clinician's scope of practice was inversely correlated to average years in practice (R<sup>2</sup> = 0.93). X-waivered clinicians indicated feeling more prepared to administer buprenorphine in the ED R<sup>2</sup> = 0.93. However, they were not more likely to report ordering buprenorphine or naloxone in the ED within the prior three months. Those who reported having a family member or close friend with substance use disorder (SUD) were not more likely to agree buprenorphine initiation is within the clinician's scope of practice (<i>P</i> = 0.91), nor were they more likely to obtain an X-waiver (<i>P</i> = 0.58) or report ordering buprenorphine or naloxone for patients in the ED within the prior three months (<i>P</i> = 0.65, <i>P</i> = 0.77). Clinicians identified availability of pharmacists, inpatient/outpatient referral resources, and support staff (peer recovery support specialists and care managers) as primary facilitators to buprenorphine initiation. Inability to ensure follow-up, lack of knowledge of available resources, and insufficient education/preparedness were primary barriers to ED buprenorphine initiation. Eighty-three percent of clinicians indicated they would be interested in additional education regarding OUD treatment.</p><p><strong>Conclusion: </strong>Our data suggests that newer generations of emergency clinicians may have less hesitancy initiating buprenorphine in the ED. In time, this could mean increased access to treatment for patients with OUD. Understanding clinician-perceived facilitators and barriers to buprenorphine initiation allows for better resource allocation. Clinicians would likely further benefit from additional education regarding medications for opioid use disorder (MOUD), available resources, and follow-up statistics.</p>","PeriodicalId":23682,"journal":{"name":"Western Journal of Emergency Medicine","volume":"25 4","pages":"470-476"},"PeriodicalIF":2.0000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11254164/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Western Journal of Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5811/westjem.18029","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Initiation of buprenorphine for opioid use disorder (OUD) in the emergency department (ED) is supported by the American College of Emergency Physicians and is shown to be beneficial. This practice, however, is largely underutilized.
Methods: To assess emergency clinicians' attitudes and readiness to initiate buprenorphine in the ED we conducted a cross-sectional, electronic survey of clinicians (attendings, residents, and non-physician clinicians) in a single, academic ED of a tertiary-care hospital, which serves a rural population. Our survey aimed to assess emergency clinicians' attitudes toward and readiness to initiate buprenorphine in the ED and identify clinician-perceived facilitators and barriers. Our survey took place after the initiation of the IMPACT (Initiation of Medication, Peer Access, and Connection to Treatment) project.
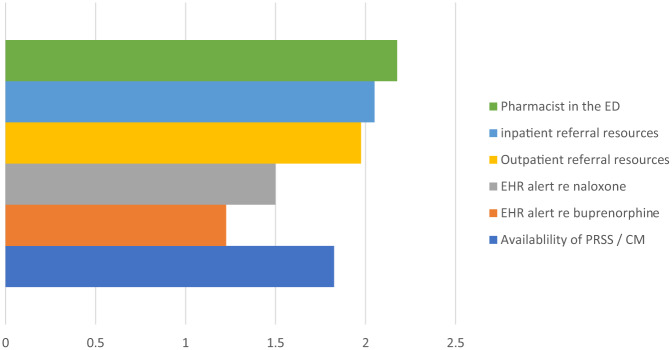
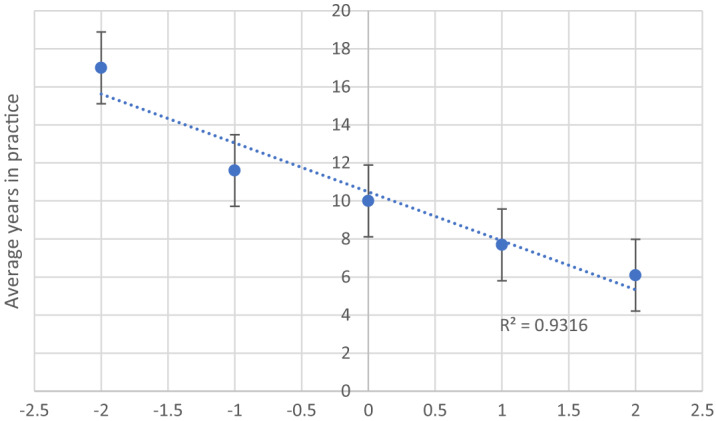
Results: Our results demonstrated the level of agreement that buprenorphine prescribing is within the emergency clinician's scope of practice was inversely correlated to average years in practice (R2 = 0.93). X-waivered clinicians indicated feeling more prepared to administer buprenorphine in the ED R2 = 0.93. However, they were not more likely to report ordering buprenorphine or naloxone in the ED within the prior three months. Those who reported having a family member or close friend with substance use disorder (SUD) were not more likely to agree buprenorphine initiation is within the clinician's scope of practice (P = 0.91), nor were they more likely to obtain an X-waiver (P = 0.58) or report ordering buprenorphine or naloxone for patients in the ED within the prior three months (P = 0.65, P = 0.77). Clinicians identified availability of pharmacists, inpatient/outpatient referral resources, and support staff (peer recovery support specialists and care managers) as primary facilitators to buprenorphine initiation. Inability to ensure follow-up, lack of knowledge of available resources, and insufficient education/preparedness were primary barriers to ED buprenorphine initiation. Eighty-three percent of clinicians indicated they would be interested in additional education regarding OUD treatment.
Conclusion: Our data suggests that newer generations of emergency clinicians may have less hesitancy initiating buprenorphine in the ED. In time, this could mean increased access to treatment for patients with OUD. Understanding clinician-perceived facilitators and barriers to buprenorphine initiation allows for better resource allocation. Clinicians would likely further benefit from additional education regarding medications for opioid use disorder (MOUD), available resources, and follow-up statistics.
期刊介绍:
WestJEM focuses on how the systems and delivery of emergency care affects health, health disparities, and health outcomes in communities and populations worldwide, including the impact of social conditions on the composition of patients seeking care in emergency departments.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
