Hye-Sol Jung, Wooil Kwon, Won-Gun Yun, Woo Hyun Paik, Sang Hyub Lee, Ji Kon Ryu, Do-Youn Oh, Kyoung Bun Lee, Eui Kyu Chie, Jin-Young Jang
{"title":"Optimal timing of surgery after neoadjuvant treatment in borderline resectable pancreatic cancer","authors":"Hye-Sol Jung, Wooil Kwon, Won-Gun Yun, Woo Hyun Paik, Sang Hyub Lee, Ji Kon Ryu, Do-Youn Oh, Kyoung Bun Lee, Eui Kyu Chie, Jin-Young Jang","doi":"10.1002/jhbp.12049","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Neoadjuvant treatment (NAT) is standard for borderline resectable pancreatic cancer (BRPC). However, consensus is lacking on the optimal surgical timing for patients with BRPC undergoing NAT. The aim of this study was to investigate the long-term outcomes of patients undergoing NAT for BRPC and suggest optimal resection timing.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Prospectively collected data for 282 patients with BRPC between January 2007 and December 2019 were retrospectively reviewed. There were 164 patients who underwent NAT followed by surgery, 45 for chemotherapy only, and 73 for upfront surgery. Among them, 150 patients who underwent R0 or R1 resection following NAT were investigated to identify prognostic factors.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Patients receiving NAT followed by surgery showed the best survival (median overall survival [OS]; NAT followed by surgery vs. upfront surgery vs. chemotherapy only; 35 vs. 23 vs. 16 months). In the NAT group, 54 (36.0%) patients received less than 3 months of NAT, 68 (45.3%) received ≥3, <6 months, and 28 (18.7%) received longer than 6 months. Patients receiving ≥3 months of NAT showed an improved OS compared to <3 months (median; not reached vs. 27 months). In the FOLFIRINOX group, patients who received more than eight FOLFIRINOX cycles showed a good prognosis (<6 vs. 6–7 vs. ≥8 cycles; median survival, 26 vs. 41 months vs. not-reached). However, >12 cycles did not carry a survival benefit compared to 8–11 cycles.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The optimal resection timing following NAT is once a patient undergoes at least 3 months of neoadjuvant chemotherapy or at least eight FOLFIRINOX cycles.</p>\n </section>\n </div>","PeriodicalId":16056,"journal":{"name":"Journal of Hepato‐Biliary‐Pancreatic Sciences","volume":"31 10","pages":"737-746"},"PeriodicalIF":2.8000,"publicationDate":"2024-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepato‐Biliary‐Pancreatic Sciences","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jhbp.12049","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Neoadjuvant treatment (NAT) is standard for borderline resectable pancreatic cancer (BRPC). However, consensus is lacking on the optimal surgical timing for patients with BRPC undergoing NAT. The aim of this study was to investigate the long-term outcomes of patients undergoing NAT for BRPC and suggest optimal resection timing.
Methods
Prospectively collected data for 282 patients with BRPC between January 2007 and December 2019 were retrospectively reviewed. There were 164 patients who underwent NAT followed by surgery, 45 for chemotherapy only, and 73 for upfront surgery. Among them, 150 patients who underwent R0 or R1 resection following NAT were investigated to identify prognostic factors.
Results
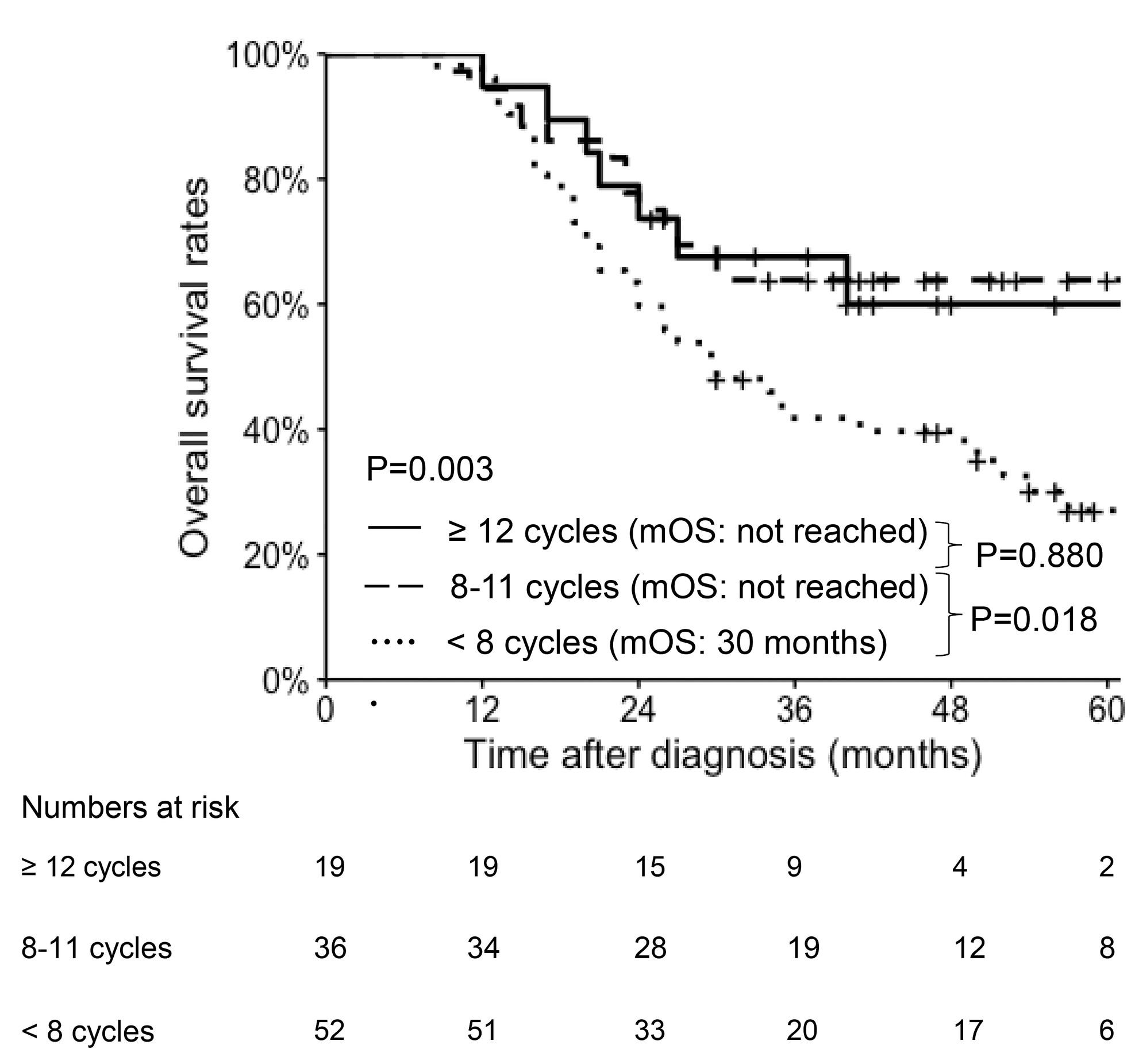
Patients receiving NAT followed by surgery showed the best survival (median overall survival [OS]; NAT followed by surgery vs. upfront surgery vs. chemotherapy only; 35 vs. 23 vs. 16 months). In the NAT group, 54 (36.0%) patients received less than 3 months of NAT, 68 (45.3%) received ≥3, <6 months, and 28 (18.7%) received longer than 6 months. Patients receiving ≥3 months of NAT showed an improved OS compared to <3 months (median; not reached vs. 27 months). In the FOLFIRINOX group, patients who received more than eight FOLFIRINOX cycles showed a good prognosis (<6 vs. 6–7 vs. ≥8 cycles; median survival, 26 vs. 41 months vs. not-reached). However, >12 cycles did not carry a survival benefit compared to 8–11 cycles.
Conclusion
The optimal resection timing following NAT is once a patient undergoes at least 3 months of neoadjuvant chemotherapy or at least eight FOLFIRINOX cycles.
期刊介绍:
The Journal of Hepato-Biliary-Pancreatic Sciences (JHBPS) is the leading peer-reviewed journal in the field of hepato-biliary-pancreatic sciences. JHBPS publishes articles dealing with clinical research as well as translational research on all aspects of this field. Coverage includes Original Article, Review Article, Images of Interest, Rapid Communication and an announcement section. Letters to the Editor and comments on the journal’s policies or content are also included. JHBPS welcomes submissions from surgeons, physicians, endoscopists, radiologists, oncologists, and pathologists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
